What is it?
- Mainly elderly (20% 65-plussers)
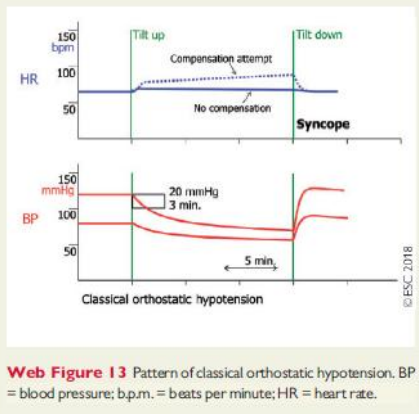
- = abnormal progressive decrease in BP upon standing (immediate or delayed)
- ≥ 20mmHg SBP OR
- ≥ 10 mmHg DBP within 3 minutes OR
- a decrease in systolic BP to < 90mmHg OR
- ≥ 30 mmHg in patients with supine HTN (>160 mmHg)
- Due to
- Low cardiac output OR
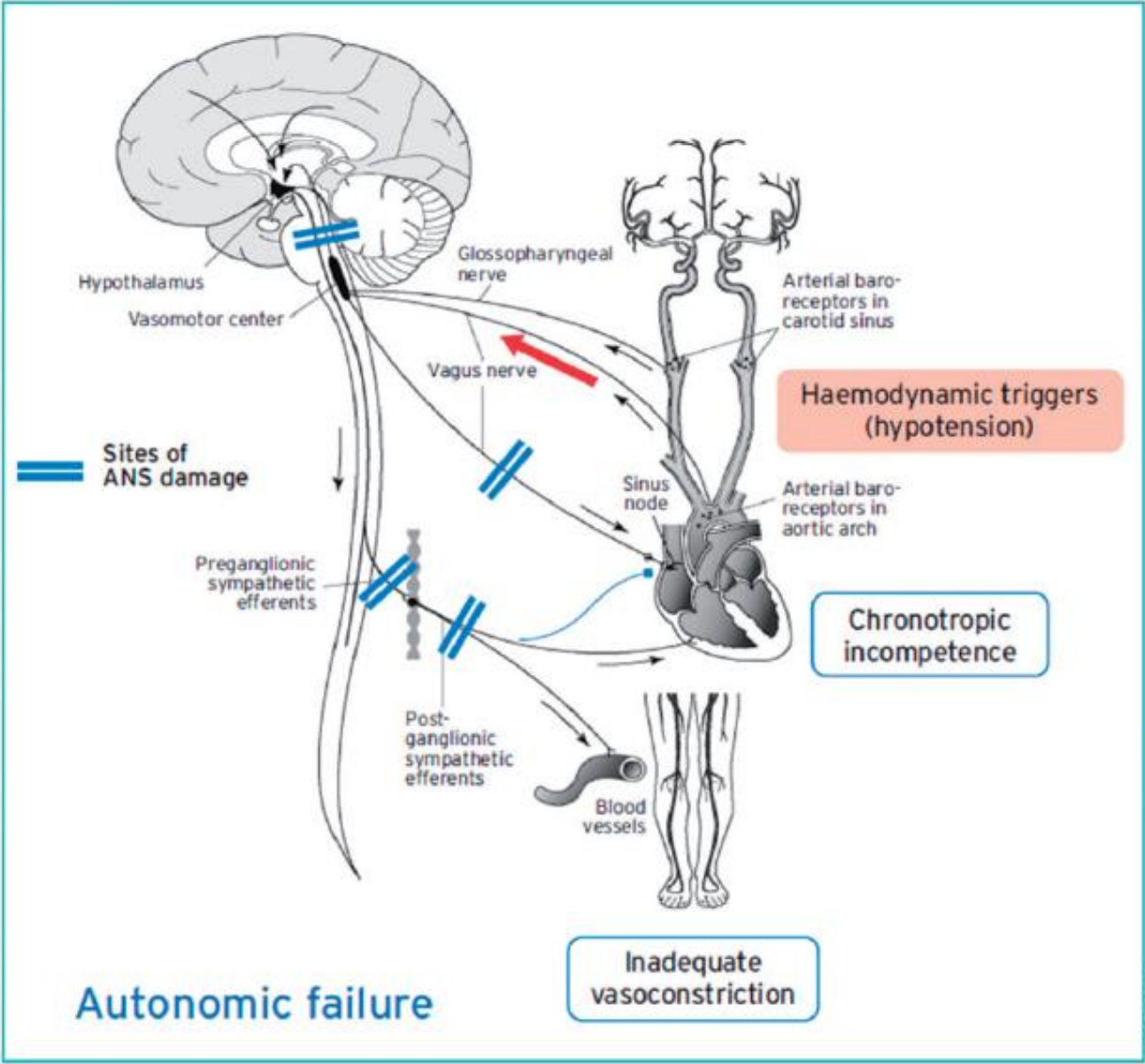
- lack of normal vasoconstriction as a results of chronic impairment of efferent sympathetic activity
Mechanism
- Low CO due to inadequate venous return
- Volume depletion
- Vomiting, haemorrhage, hyperglycaemia, diuretics
- Venous pooling: e.g. following intensive exercise
- Low SVR due to structural damage to ANS
- Primary autonomic failure:
- multiple system atrophy, Parkinson’s
- Secondary autonomic failure
- Diabetes
- Spinal cord injuries
- Amyloidosis
- Low SVR with a normal ANS
- drug-induced orthostatic hypotension
- Alcohol
- Vasodilators
- Antidepressants
Prodromal Symptoms
- Upon assuming the upright position
- Dizziness, light-headedness, pre-syncope
- Weakness, fatigue, cognitive slowing
- Visual disturbances
- Hearing disturbances
- Pain in the neck and shoulder, angina pectoris (due to ventilation/perfusion mismatching
- Skin stays WARM
Helpful hints in diagnosis of OH
- After standing up
- Documented hypotension at the event
- SBP drops at least 20 mmHg
- DBP drops at least 10 mmHg
- Or SBP < 90mmHg
- After initiating new medications
- Standing after exertion
- Prolonged standing in hot crowded places
- Worse in morning, with heat exposure or after exertion
- Positive orthostatic testing – stand up test
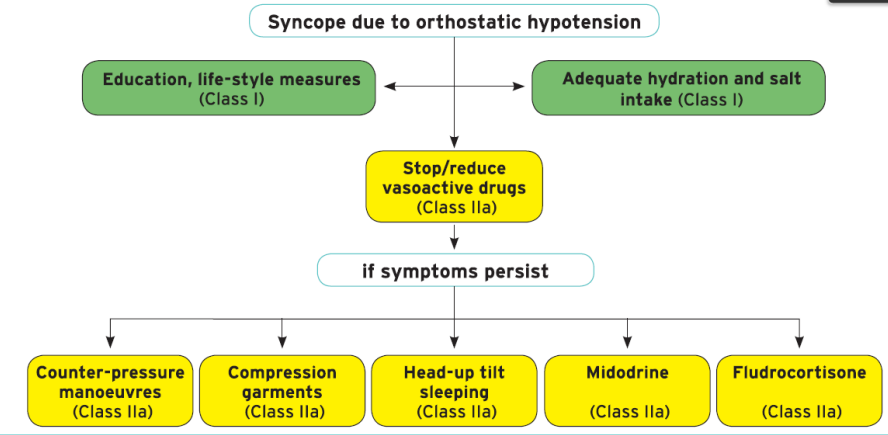
Treatment
Powered by Forestry.md