Definition
- Other terminology neurally-mediated reflex syncope
- Most common cause of syncope (especially young individuals)
- F > M
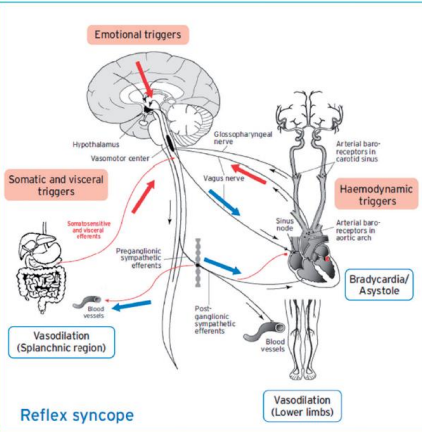
- A heterogeneous group of conditions in which cardiovascular reflexes that are normally useful in controlling the circulation become intermittently inappropriate in response to a trigger resulting in vasodilation (vaso-depression) and/or bradycardia (cardio inhibition) and hence a fall in BP
- The normal increased sympathetic tone replaced by increased vagal tone
Classification
- Neuro-cardiogenic syncope - classified according to afferent pathway
- Situational
- specific situation acts as a trigger
- cough, sneeze
- gastro-intestinal: postprandial/swallow
- post-exercise
- micturition
- specific situation acts as a trigger
- Vasovagal/common faint
- Orthostatic stressor
- triggered by prolonged orthostatic stress
- vasoconstrictor capacity is limited
- blood pooling in periphery
- Psychological stressor
- witnessing distressing accident
- pain
- instrumentation
- blood phobia
- unpleasant smell
- Orthostatic stressor
- Carotid sinus hypersensitivity
- external pressure on carotid bodies leading to symptomatic bradycardia (especially elderly, male predominance)
- head turning
- shaving
- tight collar
- 8% of elderly subjects with unexplained syncope
- external pressure on carotid bodies leading to symptomatic bradycardia (especially elderly, male predominance)
- Situational
- Classification based on efferent pathway
- Type I - mixed type (most frequent)
- Drop BP before fall in HR and
- Drop HR
-
40 bpm
- < 40 bpm for <10s without asystole
- < 40 bpm for <10s with asystole <3s
-
- Type II - cardioinhibitory type: due to bradycardia or asystole
- Drop HR
- Type 2a: <40 bpm for > 10s without asystole but BP falls first
- Type 2b: Asystole > 3s - decrease in HR before or coincides with fall in BP
- Drop HR
- Vasodepressor type: due to loss of upright vasoconstrictor tone
- Drop BP < 60mmHg
- HR does not fall more than 10% from its peak value
- Type I - mixed type (most frequent)
Hints in Diagnosis of Reflex Syncope
- Prodromes: Frequent
- almost always (i.e. autonomic symptoms) short (i.e. < 60s before fainting)
- nausea or vomiting
- feeling cold or clammy, pale
- almost always (i.e. autonomic symptoms) short (i.e. < 60s before fainting)
- Trigger
- unpleasant sight, sound, smell or pain
- Prolonged standing
- Hot crowded places / hot places
- Carotid sinus pressure: head turn, tight collar
- After exertion
- During or after heavy meals
- +/- slow fall (collapsed) from an upright position
- Short duration: 1-30 seconds
- Long history of recurrent syncope, in particular occurring before the age of 40 years
- Recovery: quickly oriented, but sometimes with persistence of nausea, pallor and diaphoresis in addition to a prolonged fatigue (minutes/hours)
Diagnosis
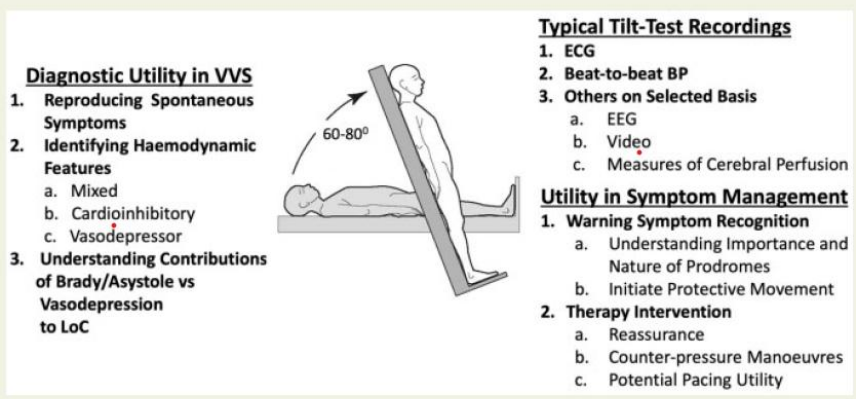
Tilt Testing

yet, it is not necessary when the clinical history is clear-cut
- Aim: INDUCE reflex syncope in patients with unexplained TLOC
- Practical:
- Fasted 4 hours prior to test
- Pre-test phase of 5 minutes
- Cannulation
- Baseline measurements
- Tilt angle: 60°
- Passive phase: 45 min standing – continuous monitoring of ECG and BP until LOC or 45 min
- Presence of cardiologist
Utility of the Tilt Test in 2025
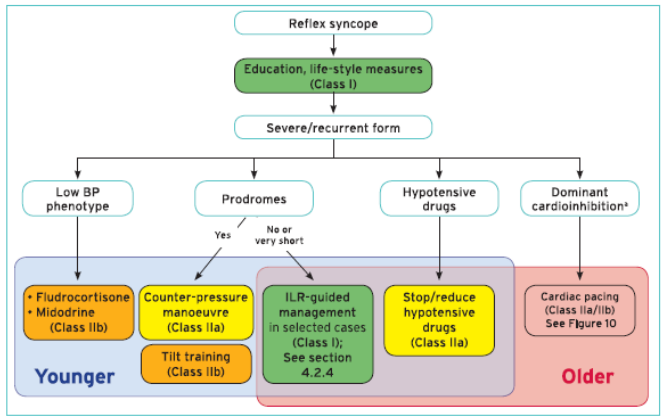
Treatment


- Reassurance of benign condition – learn to live with it
- Education & counselling = cornerstone
- Awareness and avoidance of triggers: use of cognitive behavioral therapy can be considered
- Avoidance of agents that lower BP (alpha-blockers, diuretics, alcohol)
- Salt intake: 2g
- Water intake: 2-2.5l/day
- Moderate exercise training
- Sleeping 30° head up tilting
- Early recognitions of prodromal symptoms (tilt-test can help to teach recognizing symptoms)
- Lying down
- Physical counterpressure manoeuvres
- Leg Crossing
- Hand gripping
- Arm tensing
- isometric contractions
- increase BP
- increase cardiac output
- isometric contractions