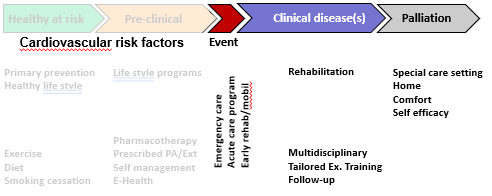
- It is marked by an event (super-acute phase)
- future stroke should be prevented.
- There are multiple factors that impact rehabilitation
- Medical Factor
- Significance of the stroke
- Comorbidities
- Neurologic deficit (paralysis, aphasia, dysphagia, cognitive impairment)
- Pain and spasticity
- Fatigue (physical and mental)
- Depression and anxiety
- Psychosocial factor
- Low social support —> complex rehab
- Motivation and adherence
- Cognitive and mental health issues
- Rehabilitation landscape and environment
- Access to care
- Quality of care
- Financial problems (e.g. therapy and assistive devices)
- Accessibility of the home environment
- Medical Factor
Exercise training after stroke
- Movement become inefficient after stroke.
- Residual impairments caused by the stroke
- Hemiparesis
- Spasticity
- Cognitive dysfunction / Depression
- Aphasia
- Poor ‘mechanical’ efficiency and low fitness making PA more difficult.
- Residual impairments caused by the stroke
- Reluctance to engage in exercise due to lack of awareness of exercise feasibility, lack of specialist
- Awareness that exercise is feasible or desirable,
- Access to resources to support exercise,
- Structured exercise sessions whereby exercises could be demonstrated by a rehabilitation specialist or exercise leader
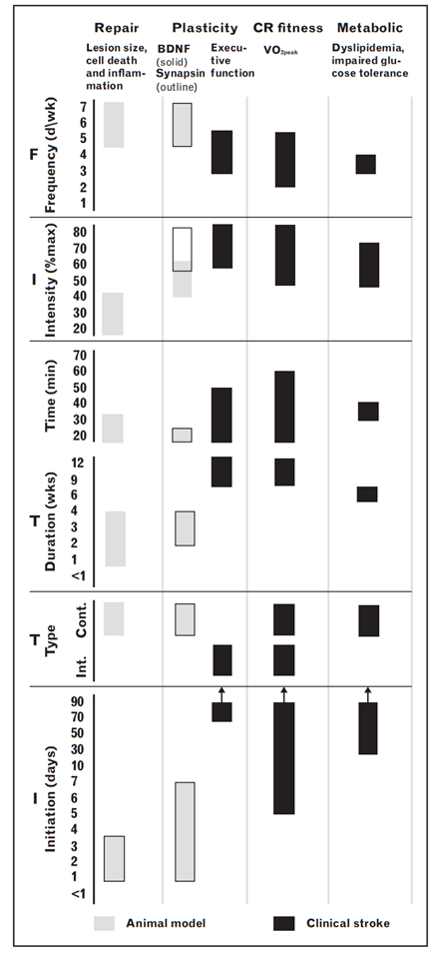
- The earlier the exercise is initiated, the better the repair of the brain lesion will be (imp to start early)
-
8 weeks, >20mins program, progression and sustained PA after the end of the program
Effect of exercise training in stroke
- Immediately after acute stroke
- Medically stable
- Regaining PF
- Long term secondary/tertiary prevention
-
- How to maintain a PA lifestyle and preventing a risk of another stroke.
-
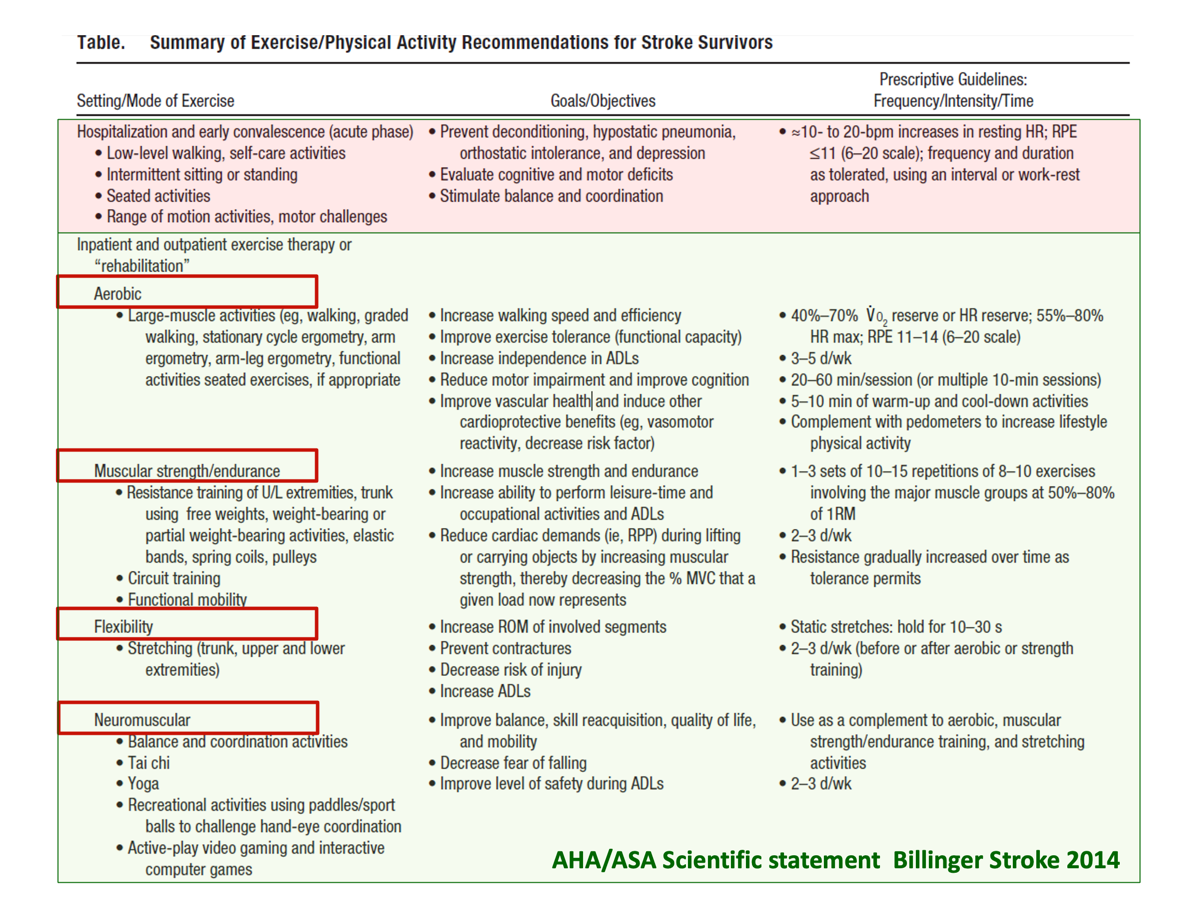
Evidence for exercise training in stroke
- There will be an increase of 1 MET with Aerobic training
- 33m improvement in 6MWD (MCID for stroke is around 70m)
- In respiratory, it is around 30m
- It is safe to perform aerobic training (or any other training programs) as many patients have went through such programs.
- It is important to specify the program (walking should be specified with intensity, stair climbing)
Implementation of exercise training in Stroke
- Screening assessment to identify medical conditions - Recommended
- General information including
- demographics, medical history, medications, cardiac history, seizure history, diabetes control, lifestyle habits
- General information including
- Assessment of contraindications to exercise testing and training
- Evaluate motor function, mobility, balance, swallowing, cognition and communication
- Incremental exercise test is recommended.
- up to 75% of stroke victims have coexisting cardiac disease and 20-40% of asymptomatic stroke patients may have abnormal tests for silent cardiac ischemia, an incremental exercise test is recommended.
- If it is not available, it is recommended to however start and initiate the training program. But, it will be difficult to monitor and prescribe intensity
- 6MWD can be prescribed.
- Acute in pink and Medically stable in green
- Isometric exercises can be given in acute case, but more functional exercises to be prescribed later.
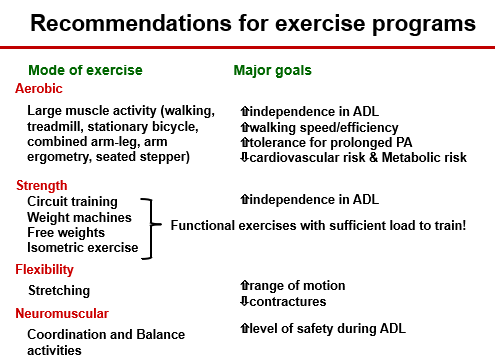
Recommendations for exercise programs
Special Consideration
- Monitor cardiovascular safety, HR (is there a irregular rhythm)
- Medications that affect the exercise program
- Modification of exercise devices (pedals on bikes)
- They would not usually feel the impairment or injury