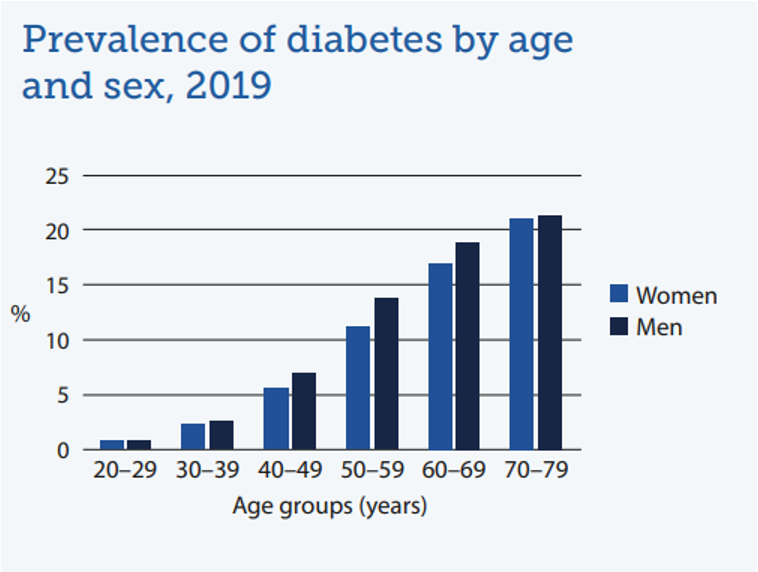
- It was presumed as a disease for elderly, but recently has been changed, and it could happen in younger age.
- In Belgium 1/15 adults has (type II) diabetes
- Prevalence increases with increasing age
- In Flanders in 2018 : 58 people / 1000 inhabitants are treated for diabetes
- Type I diabetes: Generally auto-immune destruction of pancreatic beta cells
- Type II diabetes: Reduced insulin sensitivity of tissue
Diabetes mellitus is characterized by hyperglycemia
- Fasting plasma glucose level at or above 126 mg/dL (7.0 mmol/l).
- Any body part with high capillaries could be damaged
Type I Diabetes, Glucose management…
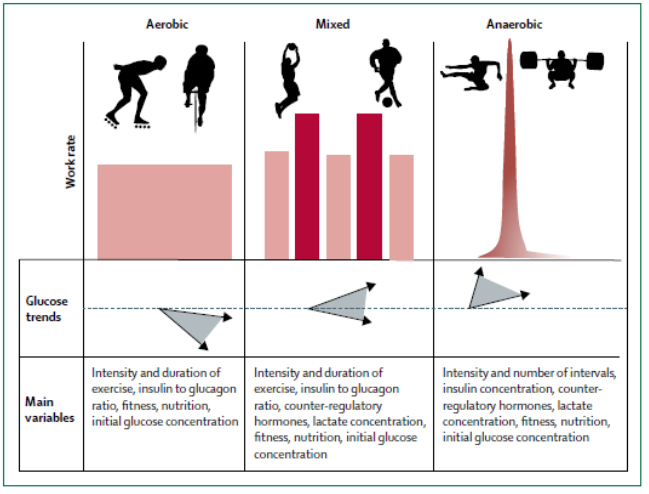
- In mixed sports, glucose could go up or down. It is imp to monitor blood glucose with ppl performing such sports.
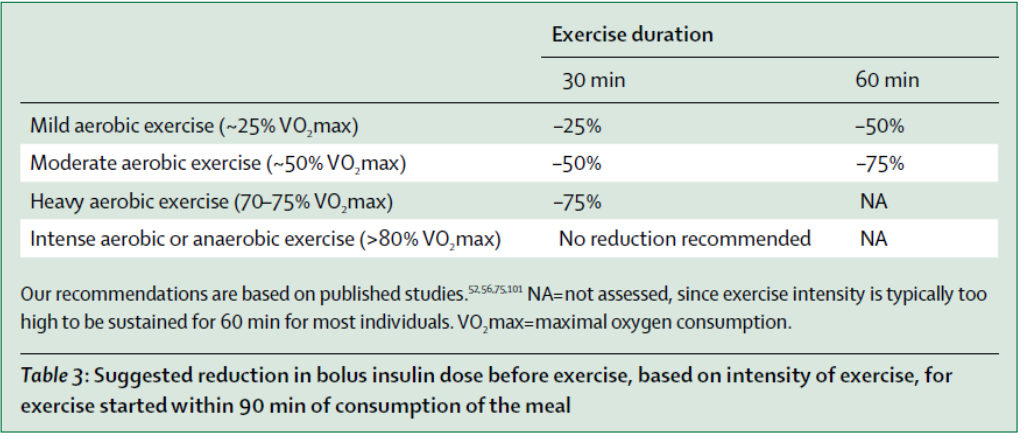
- Pre-workout: Ingest glucose
- During workout: check ketones, and it is elevated—> perform only mild exercise.
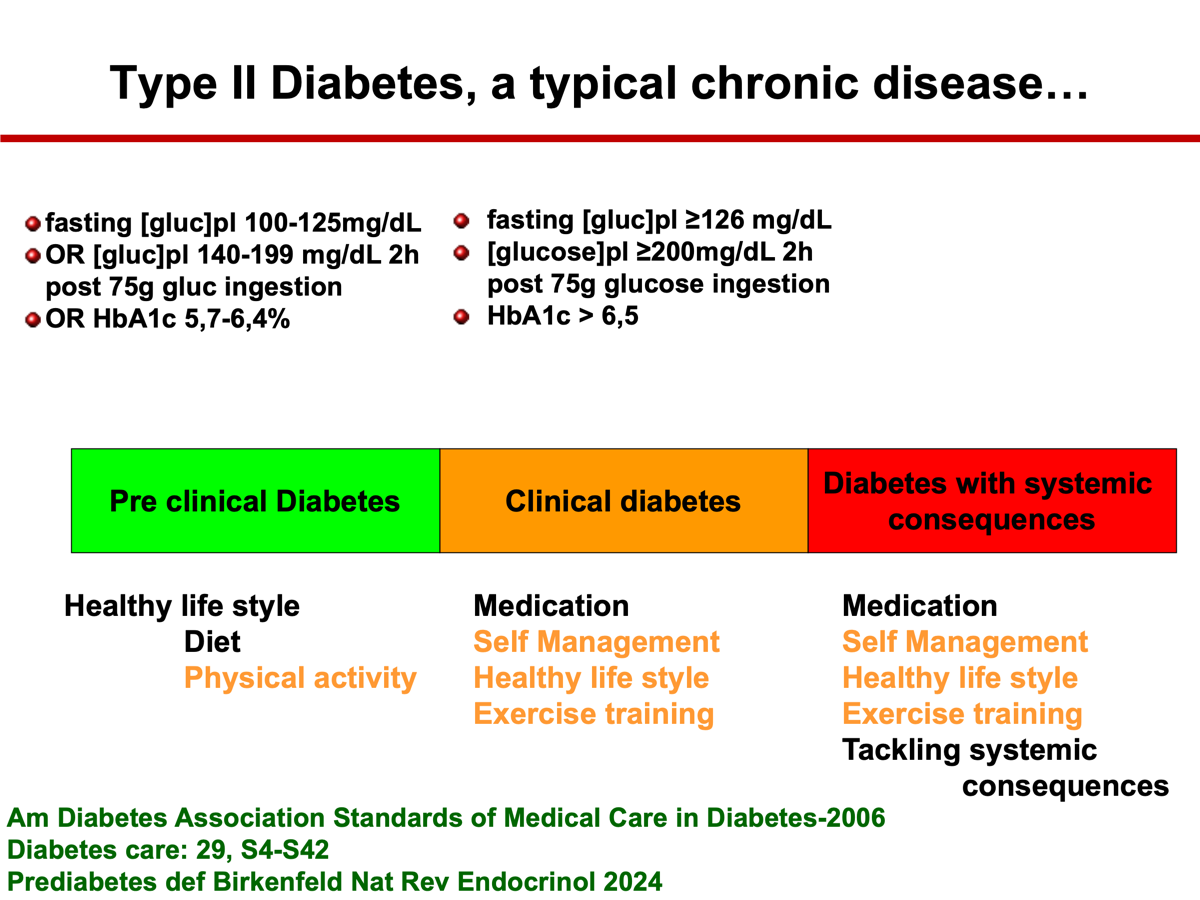
Type II Diabetes, a typical chronic disease…
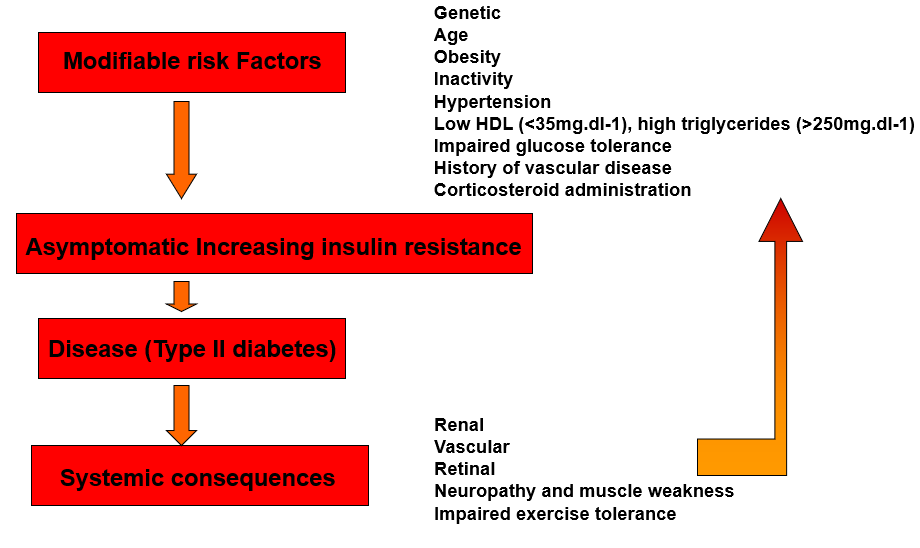
- Patients with chronic corticosteroid use would develop Type II diabetes in the future.
- Muscle weakness is seen in late stages
- Management gets harder with progression of the disease.
Pre-clinical Diabetes:
- Awareness of the modifyable risk factors
- Active counseling (diet, PA) if impaired glucose tolerance or impaired fasting glucose
- Adequate follow-up
- Follow-up every 1-2 years
- Attention for other CVD risk (tobacco, hypertension, dyslipidemia)
- Drug therapy is not routinely needed
- Self management of PA/diet
Clinical diabetes
- Medication
- Self Management and education
- Self monitoring of glucose
- Healthy life style
- Medical nutritional therapy
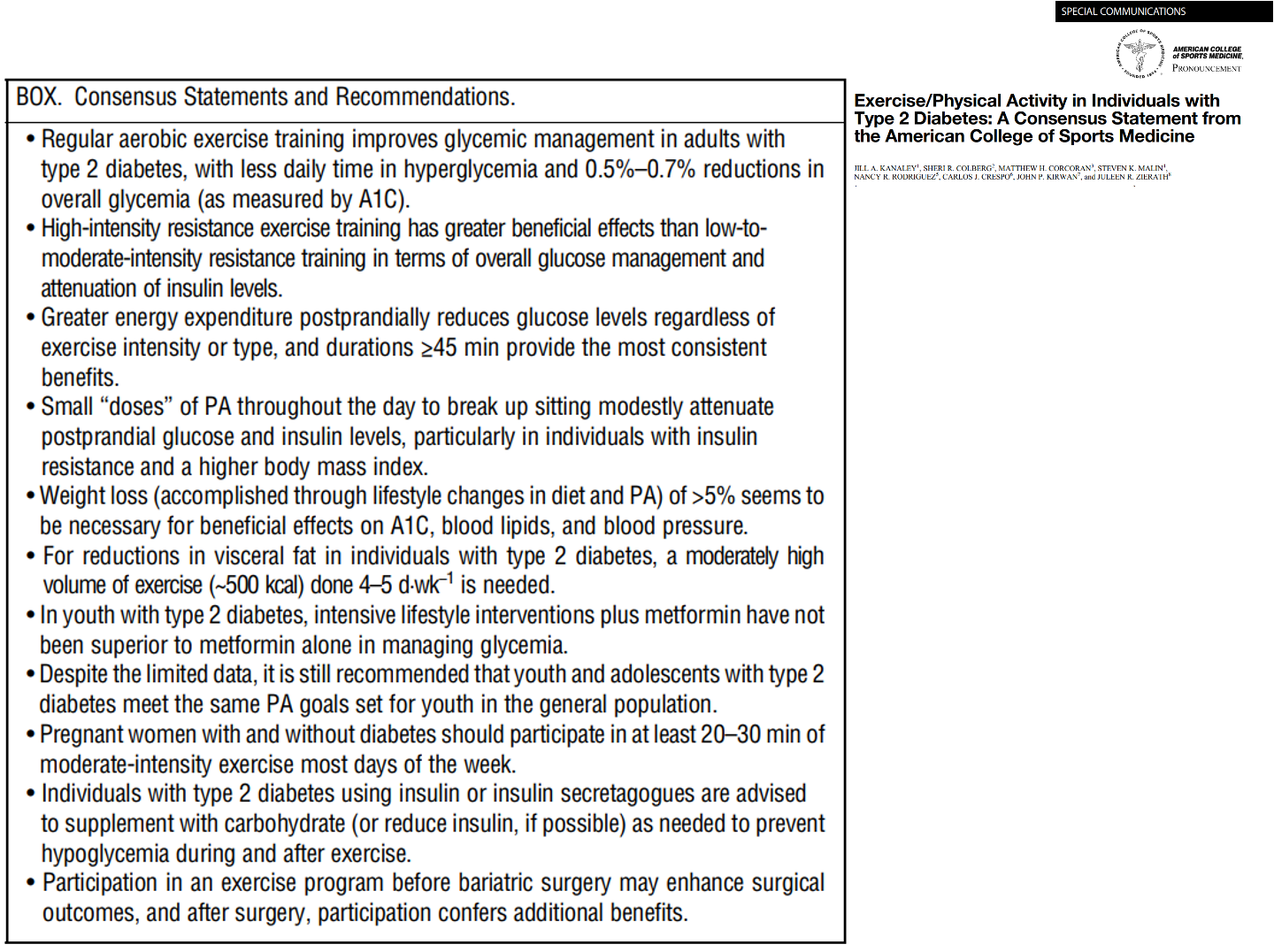
- Exercise training /Physical activity
- PA > 150min/wk of moderate intense PA
- and/or 90min of vigorous PA
- not more than 2 consecutive days without PA
- Resistance training 3/wk
- An exercise test is needed
- Vigorous activity should be avoided in the presence of ketosis (Hyperglycemia)
- Pay attention to hyperthermia when sports on warm days
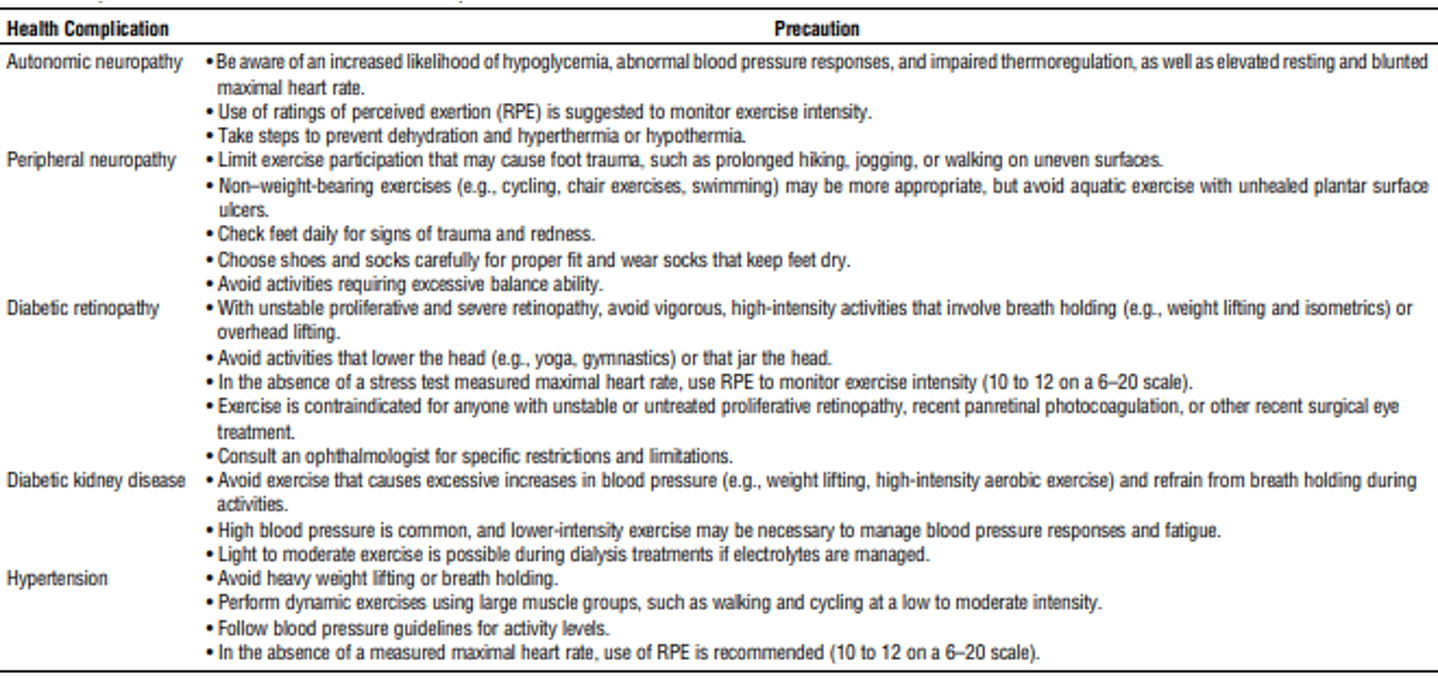
Diabetes with systemic consequences
- In patients with proliferative diabetic retinopathy
- vigorous aerobic or resistance exercise may be contra-indicated (hemorage and retinal detachement)
- Peripheral neuropathy
- Decreased pain sensation-> skin irritation
- Charcot joint destruction
- In severe peripheral neuropathy, non- weight bearing activities (swimming, cycling, arm exercises)
- Autonomic neuropathy
- decrease in cardiac responsiveness to exercise, postural hypotension, decrease thermoregulation (decrease skin blood flow/sweating), decrease night vision, increase risk of dehydratation, increase risk gastroparesis (food delivery not guaranteed)
- Foot ulceration “diabetic foot”
- In these patients thorough CV assessment is imperative!
Resistance training in diabetes
(Gordon Diabetes research and clinical practice 2009.)
- Duration Median 16wk (range 8-52)
- Machine weights, 1 free weights, 1 NR
- Frequency 3/wk 3x8reps (n=6) other regimens (n=5)
- Improved glycemic control (potentially superior to AT) particularly if duration > 10Wks
- Improved skeletal muscle function, and counteracts hypocaloric diet induced loss of muscle strength
- Systematic review: High intensity resistance exercise (75-100% 1RM)seems to improve glycemic control more than low-mod intensity resistance training (20-75%1RM)
Points of attention during exercise
- Hypoglycemia
- Shaking trembling
- Sweating (‘cold sweat’), weakness
- Tachycardia, tingling fingers
- Hunger
- Dizziness (lightheaded)
- Blurred vision
- Irritability (or sudden mood change, anxiety)
- Difficulty concentrating
- Confusion, difficulty speaking, poor coordination, loss of consciousness, seizures
- Hyperglycemia
- Excessive thirst
- Polyuria
- Fatigue
- Blurred vision
- Dry mouth
- Diabetic ketoacidosis (fruity-aceton smellingbreath, rapid breathing, drowsiness)
- When prolonged: Nausea, vomiting, abdominal pain, weight loss, slow wound healing, recurrent infections.