Pain catastrophizing is characterized by the tendency to magnify the threat value of a pain stimulus and to feel helpless in the presence of pain, as well as by a relative inability to prevent or inhibit pain-related thoughts in anticipation of, during, or following a painful event.
People who catastrophize tend to do three things:
They ruminate about their pain (e.g. "I can´t stop thinking about how much it hurts")
They magnify their pain (e.g. "I´m afraid that something serious might happen")
They feel helpless to manage their pain (e.g. "There is nothing I can do to reduce the intensity of my pain")
How is it observed?
In physiotherapy practice
frequent reporting/talking of pain
nervousness or anxiety
appearing hopeless
limiting active involvement in the exercise you provide due to fear of exacerbating pain
screaming or using profane language when having pain sensations while exercising
To measure or not?
NO:
Physiotherapists may feel that they are treading outside their scope of practice
Patients with chronic pain may be concerned about being stigmatised or labeled as malingerers
YES:
Addressing psychosocial factors is essential in the recovery process and will minimise daily life limitations
A non-judgmental therapeutic approach can help prevent having the feeling of being stigmatised and labeled
Questionnaires are simply a means of gaining insight into the thoughts and feelings that patients associate with pain.
Elevated scores of pain catastrophizing and pain related fear are not grounds for discharge from physiotherapy.
Rather, they should be used as criteria for implementing targeted interventions such as education, activity encouragement, graded exposure, graded activity
How to talk about pain catastrophising in physiotherapy?
Setting the stage
In recent years, we have learned that how we think about pain affects how we feel and respond to it
It is normal to have concerns when dealing with pain
Communicating as a physiotherapist
When we are in pain, our brain can go into overdrive - like it is sounding the alarm too loudly
It is understandable. When pain lingers, it can be very stressful and tiring
Our thoughts can shape our experience of pain. When we are caught thinking the worst and feeling that we cannot cope, it can affect our recovery.
Emphasising collaboration
What do you think about completing a few questions or a brief questionnaire? It would tell me more about what you are experiencing and how your pain is affecting you.
Assessment of pain catastrophising
The Pain Catastrophizing Scale (PCS) (Sullivan, 1995) is the most widely used in the world.
It consists of 13 items describing different thoughts and feelings that people may have during painful episodes.
Participants are requested to rate how frequently they experienced specific thoughts and feelings when they experience pain using a 5-point scale (0 ='not at all', 4 ='all the time’).
The PCS consists of three subscales
(1) rumination (e.g., '... I keep thinking about how much it hurts’),
(3) helplessness (e.g., '... there is nothing I can do to reduce the pain’).
1, 2, 3, 4, 5, 12
Back to Kinesiophobia or Fear of movement
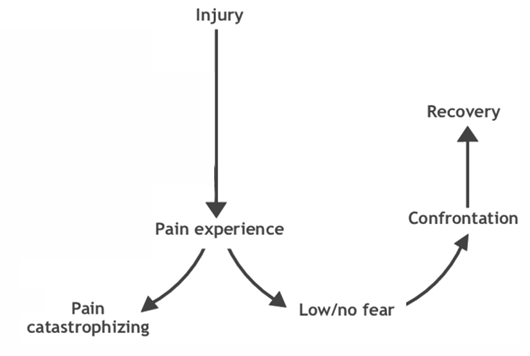
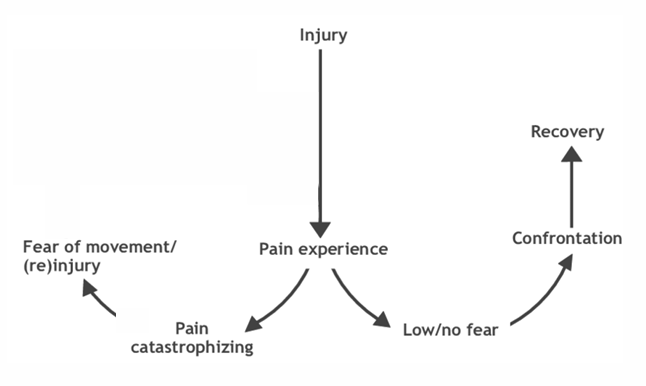
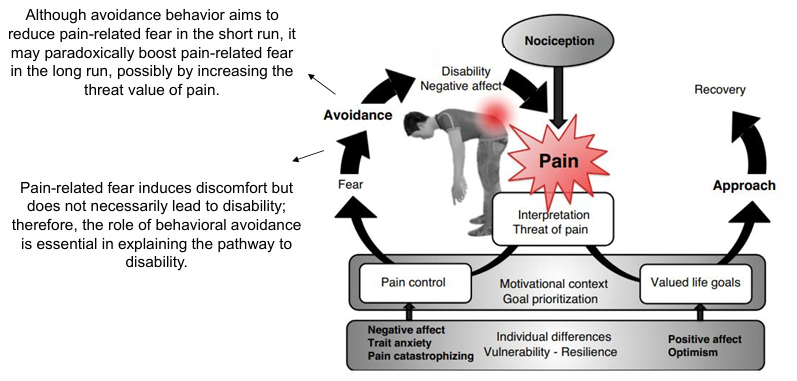
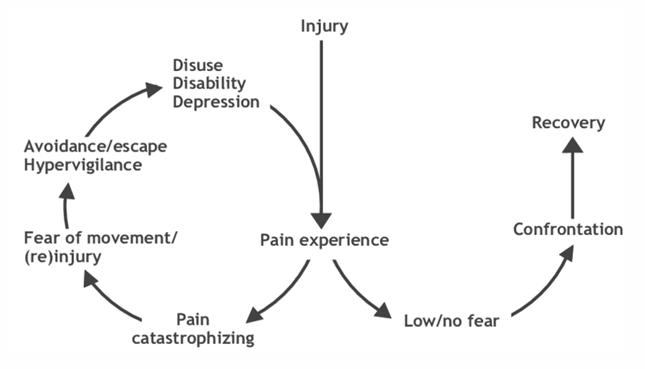
Catastrophic misinterpretations of pain as being harmful may give rise to pain-related fear, which in turn can initiate avoidance behavior intended to avert bodily threat.
When such a protective action serves to reduce genuine bodily threat (such as in acute pain), it is highly adaptive, but when pain persists beyond healing time and turns chronic, it may paradoxically increase suffering and disability
How to talk about the Tampa Scale of kinesiophobia in physiotherapy?
Setting the stage
It is normal to feel cautious or worried about moving after an injury
Communicating as a physiotherapist
Sometimes, after an injury, it is easy to worry that moving will make the pain worse or cause more damage - out body gets "stuck in caution mode"
It is natural to be concerned about re-injury, but avoiding movement can lead to more stiffness and weakness
Take it slowly. My goal is to help you gain confidence in moving again without feeling like you have to protect everything
Reflecting concerns
I have noticed that you seem hesitant about moving, like it is tough to even think about trying some activities right now
Seeking patient insight
How would you feel about answering a few questions that might give me a better understanding of how fear of movement is affecting you?
Tampa Scale of Kinesiophobia
The TSK (Miller et al., 1991) is a 17-item self report checklist using a 4-point Likert scale (from strongly disagree to strongly agree) that was developed as a measure of fear of movement or (re)injury.
The scale has two sub-sales:
Activity avoidance – the belief that activity may result in (re)injury or increased pain.
Somatic focus – the belief in underlying and serious medical problems
A high value on the TSK indicates a high degree of kinesiophobia, where a score of 37 or over is considered as a high score and predictive of poorer health outcomes.
Use of a total score (including all 17 items) is recommended, although practitioners may wish to interpret results using two subscales
Items 4, 8, 12 and 16 are being reversely scored
Activity avoidance: items 1, 2, 7, 9, 10, 11, 12
Somatic focus: items 3, 4, 5, 6, 8
The other items are "rest" items to measure overall kinesiophobia symptomatology
How to approach pain catastrophising and kinesiophobia in your physiotherapy session?
CBT is evident that it helps with kinesiophobia
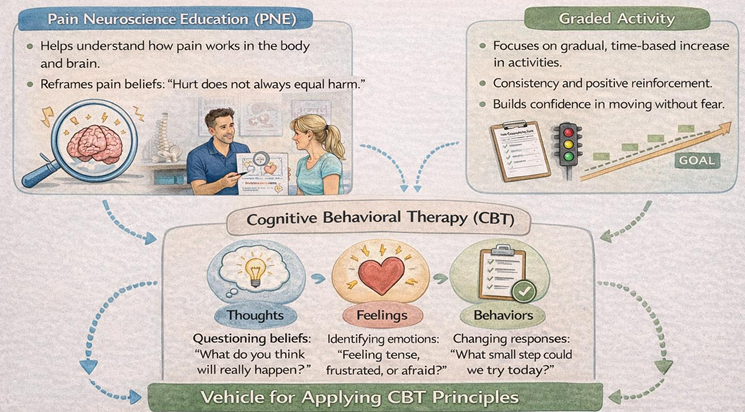
Combining Pain Neuroscience Education with Graded Activity as a Vehicle for Applying CBT Principles
Graded activity is a type of CBT. It is a complementary to physical activity
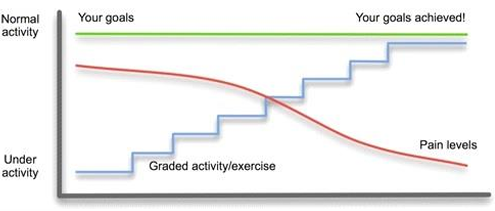
Avoiding avoidance and gradually increasing activity again
Activity is increased in step-wise
We are not focusing on Sx and lead by feeling of pain, and asking about pain should be avoided and asked less.
Just acknowledge them
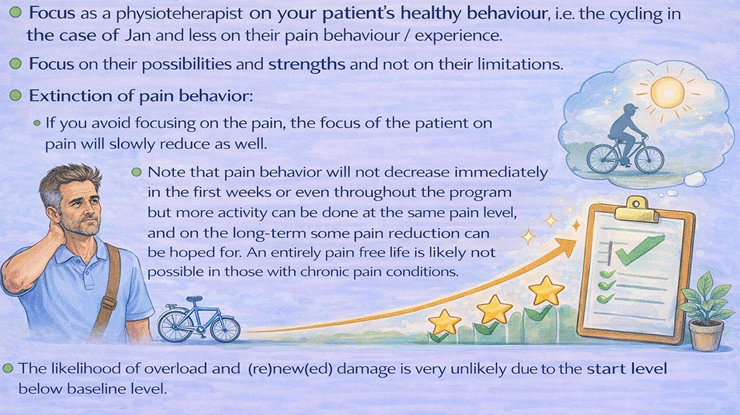
Explain at the beginning what as a PT you will do and that pain is important in your life, but we want to increase your function and activity but not driven by pain.
"Do not worry if there is pain, we are below the baseline and threshold of pain and we aim to increase your PA"
Also, we do not believe that pain would decrease at the beginning of the intervention.
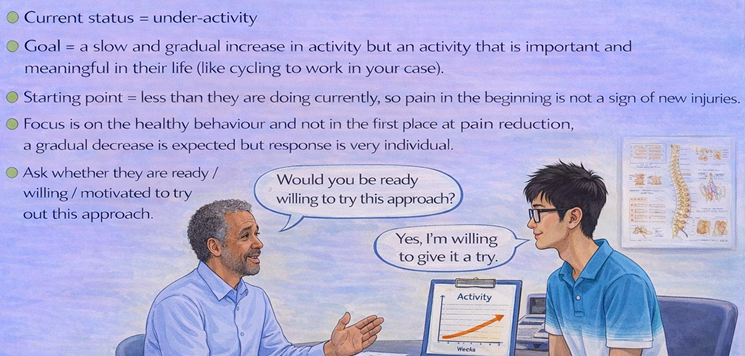
Step 1: Setting a baseline
Always, set a baseline, and then we work below that level
Always start with assessing by recording their ADL.
Assessment is not about screening but education too.
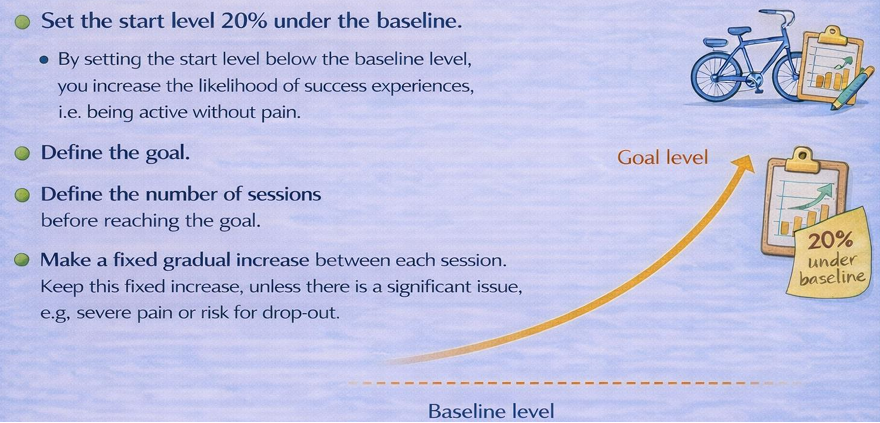
Step 2: Setting the start level and goal
Know that there could be a relapse.
Start at baseline -20%
Check if these patients are motivated—collaborative care
Define the gradual increase
Step 3: Action stage
In action stage, focus on activity and patient's healthy behaviour.
In offday, if pain was bad, explain that it is normal.
In relapse, it is rare to change the plan, rather focus on the barriers, and learn from the set backs.
Graded Activity
How to explain the rationale to your patient?
Evidence for chronic pain
Graded activity reduces disability in people with chronic low back pain (Ibai 2016)
But do graded acitivty therapies harm in chronic fatigue syndrome (
More and more evidence becomes available that graded activity should be avoided in chronic fatigue syndrome.