Implementing cognitive behavioural aspects in treating compulsive exercise within physiotherapy
It is concerned principally with the present and future rather than the past.
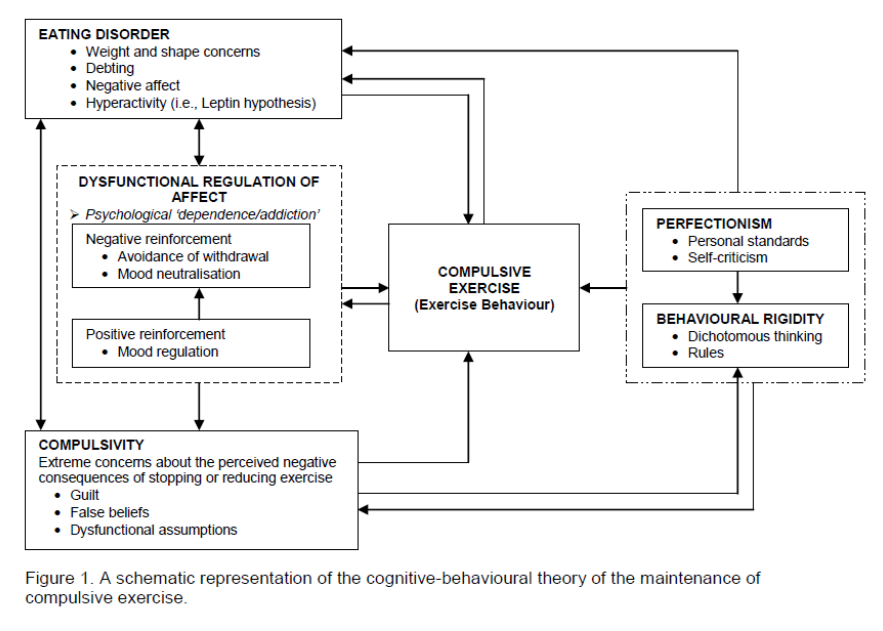
The focus is on those factors and processes that maintain the exercise behaviour.
It should be very much an “active” therapy, with responsibility for behaviour change residing with the patient.
Exposure therapy
The therapist’s role is to provide information, guidance, support, and encouragement.
It is essential that a trusting, collaborative relationship is established.
Aims of a cognitive behavioural approach
To educate the patient about the cognitive view on the maintenance of compulsive exercise.
To promote insight into the factors affecting (maintaining) the patient’s attitudes, beliefs and behaviours toward exercise.
To educate the patient about what constitutes „healthy‟ exercise.
To introduce the patient to the cognitive skills and strategies necessary to challenge maladaptive attitudes, beliefs and behaviours toward exercise.
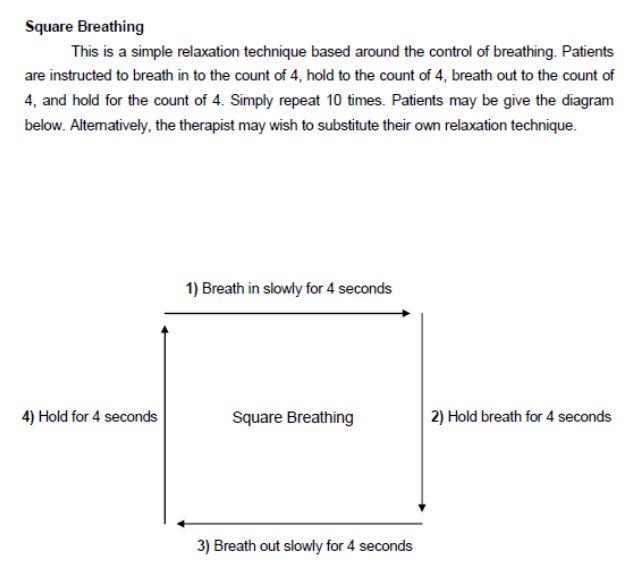
To introduce the patient to alternative (adaptive) emotion coping strategies.
To educate the patient about relapse prevention.
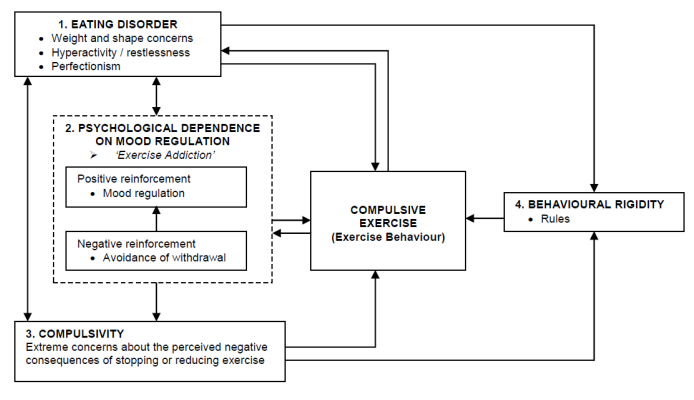
Negative reinforcement:
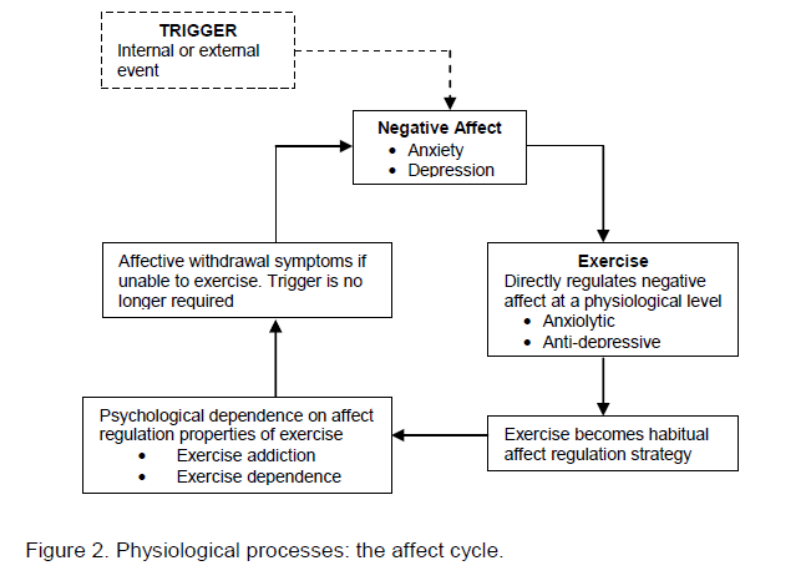
Compulsive exercisers experience affective withdrawal symptoms when they are unable to exercise (e.g. anxiety, depression, guilt, irritability, frustration, anger), and avoidance of these adverse symptoms is a primary maintaining mechanism for the exercise behaviour (i.e., negative reinforcement).
Positive reinforcement:
Exercise is not always a dysfunctional behaviour in terms of affect regulation. It may be an adaptive way of regulating affect.
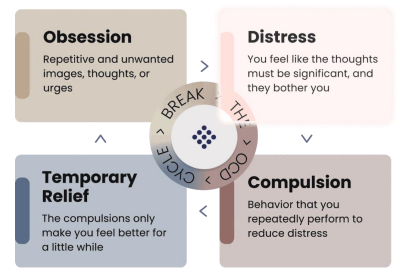
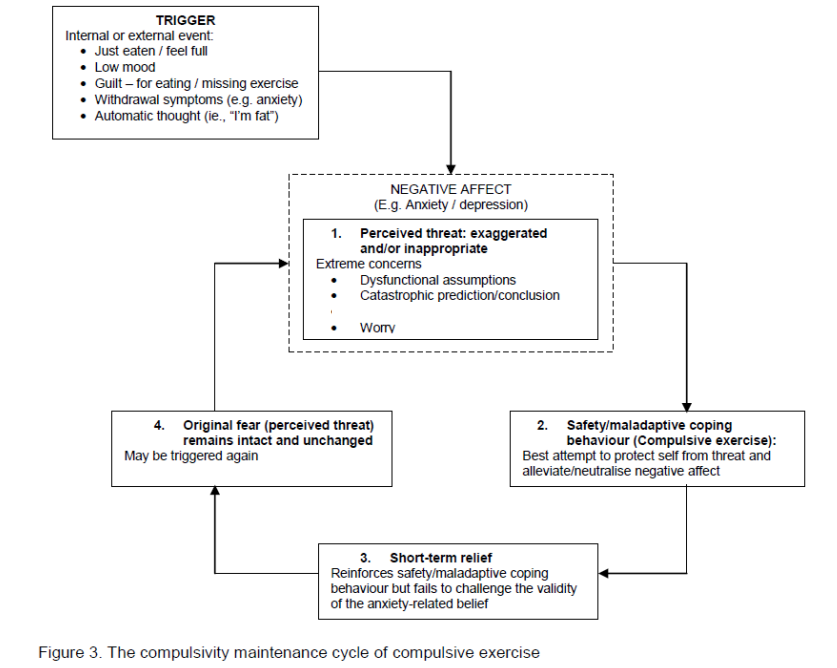
Compulsivity:
Triggers the "OCD" cycles
OCD cycle
Start of a CBT approach in your physiotherapy setting
Education and assessment
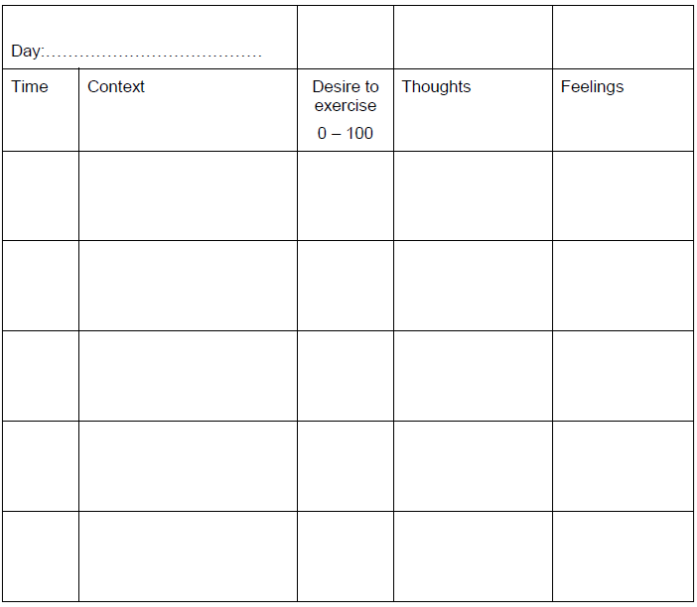
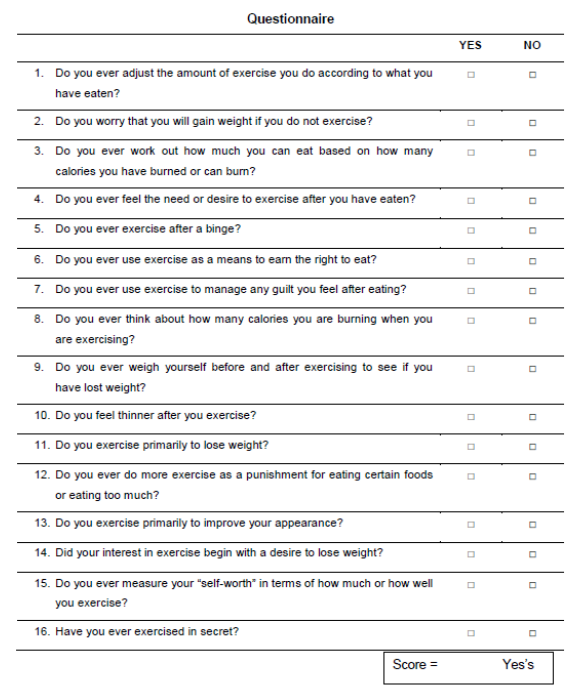
Homework: monitoring
Monitoring is a way of recording the things that have an influence on patients’ behaviour and it can provide a detailed picture why they behave a certain way.
The reason to use a monitoring sheet is that it can help to examine and understand the role thoughts and feelings play in making patients to behave a certain way.
It makes them more aware of what they are doing and why they are doing it.
Monitoring is a very powerful way of helping to change behaviour that previously seemed automatic or even out of patients’ control.
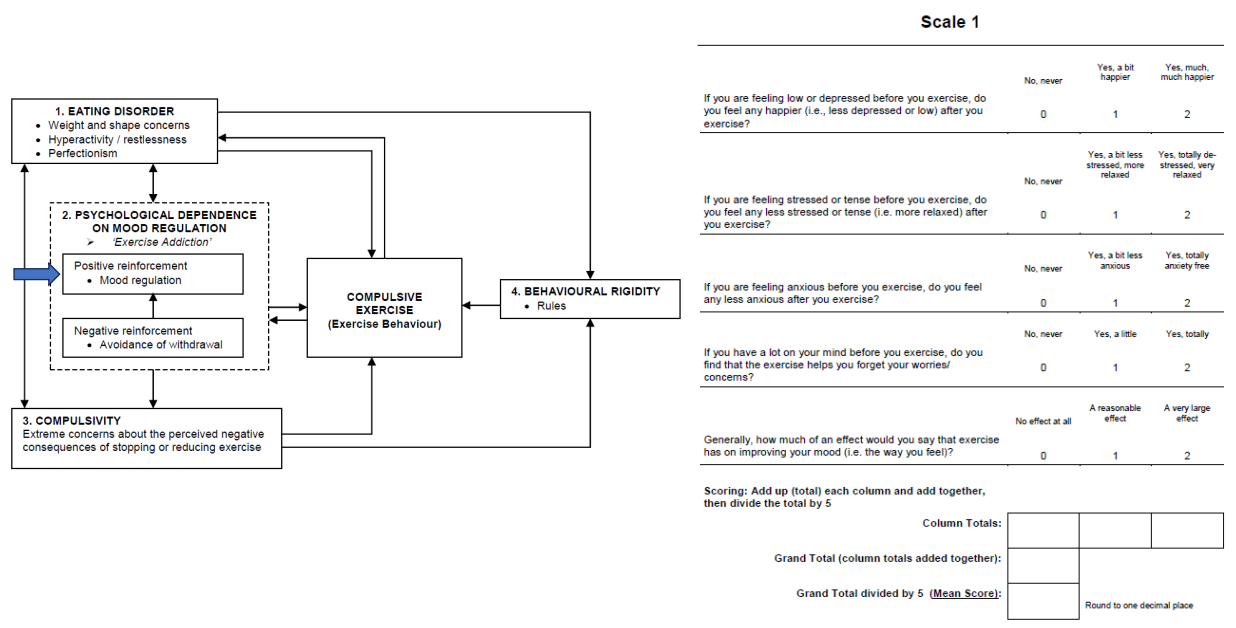
Mood improvement / positive reinforcement
This scale measures how much of a positive effect exercise has on a patient’s mood.
A high score:
A substantial mood improvement as a result of exercising -> exercise = reinforcing.
Susceptible to becoming psychologically dependent on exercise as a means to improve or regulate mood (see scale 2).
Likely difficulties to cut down or stop exercise behaviour.
A mid-range score:
A positive uplift in mood as a result of exercising, but unlikely to be psychologically dependent on exercise as a means to improve or regulate their mood.
A low score:
Exercise has little to no effect on mood: exercise is probably not a very pleasurable activity.
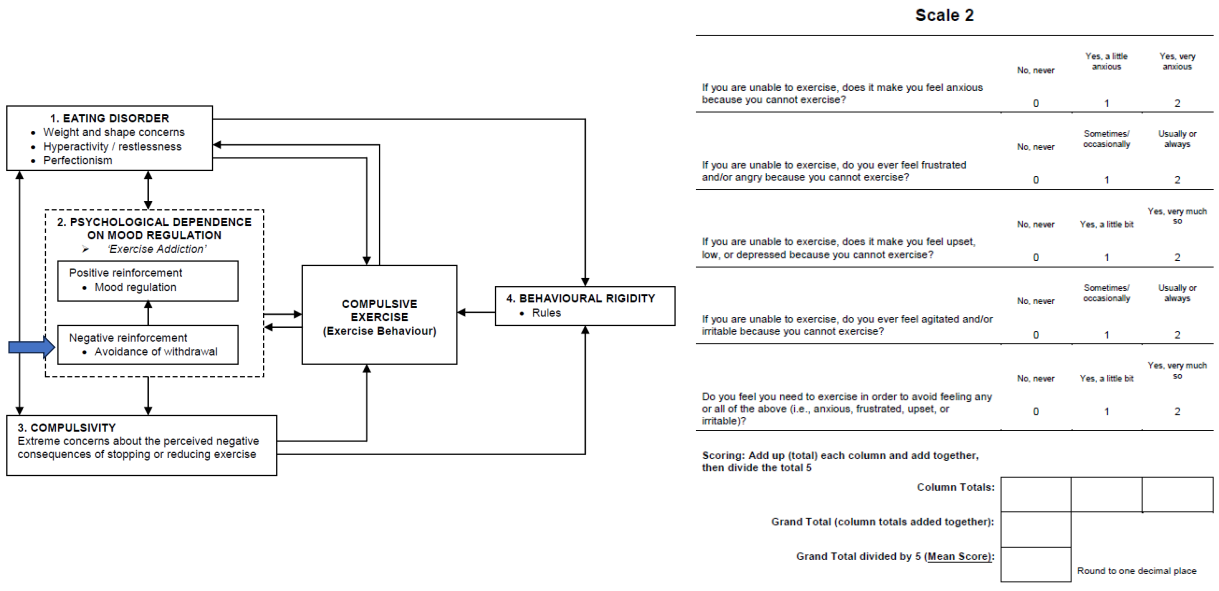
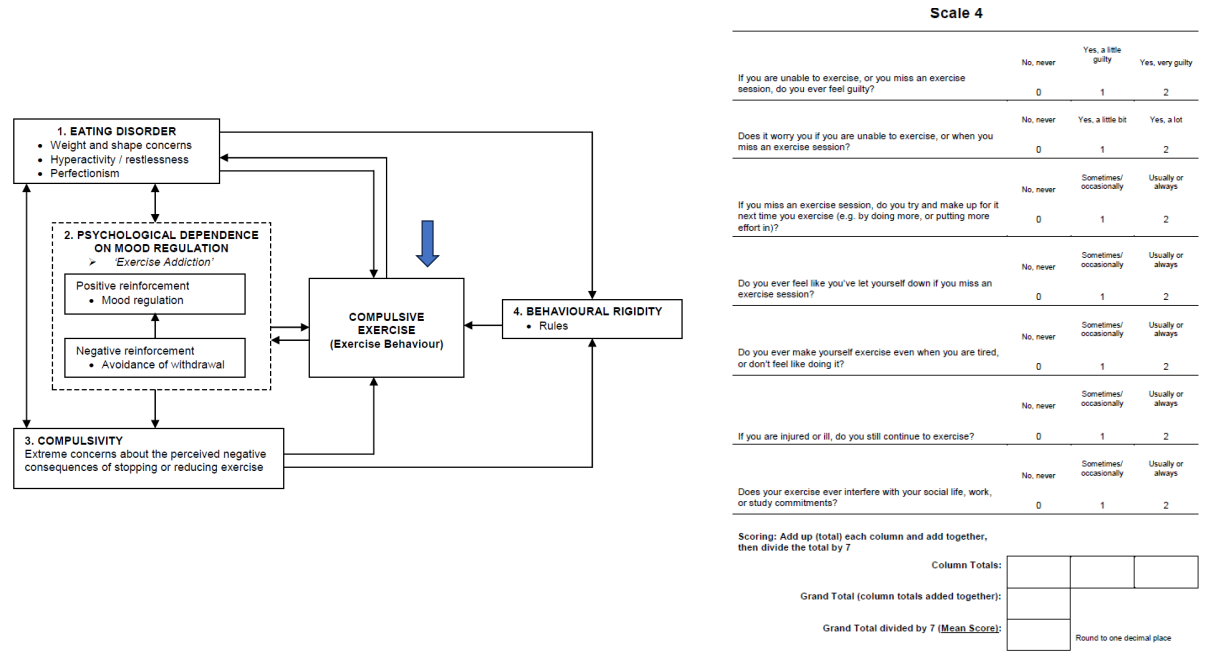
Negative reinforcement (mood avoidance)
This scale measures the effect on a patient’s mood of being unable to exercise.
It is a measure of dependence on exercise as a means of avoiding (regulating) negative emotions (an avoidant coping mechanism).
A high score:
Exercise = a means of avoiding (regulating) a wide range of negative mood states or emotions -> a high level of psychological dependence on the mood regulatory effect of exercise.
Likely very difficult to cut down or stop exercise (withdrawal symptoms).
A mid-range score:
Either psychologically dependent on exercise as a means of avoiding/regulating certain specific negative mood states or „at risk‟ of developing a psychological dependence on exercise.
Likely quite difficult to cut down or stop exercise behaviour.
A low score:
Exercise is not used as an avoidant coping mechanism -> not psychologically dependent on exercise as a means to regulate your mood, -> able to stop or cut down exercise behaviour without suffering a negative mood state.
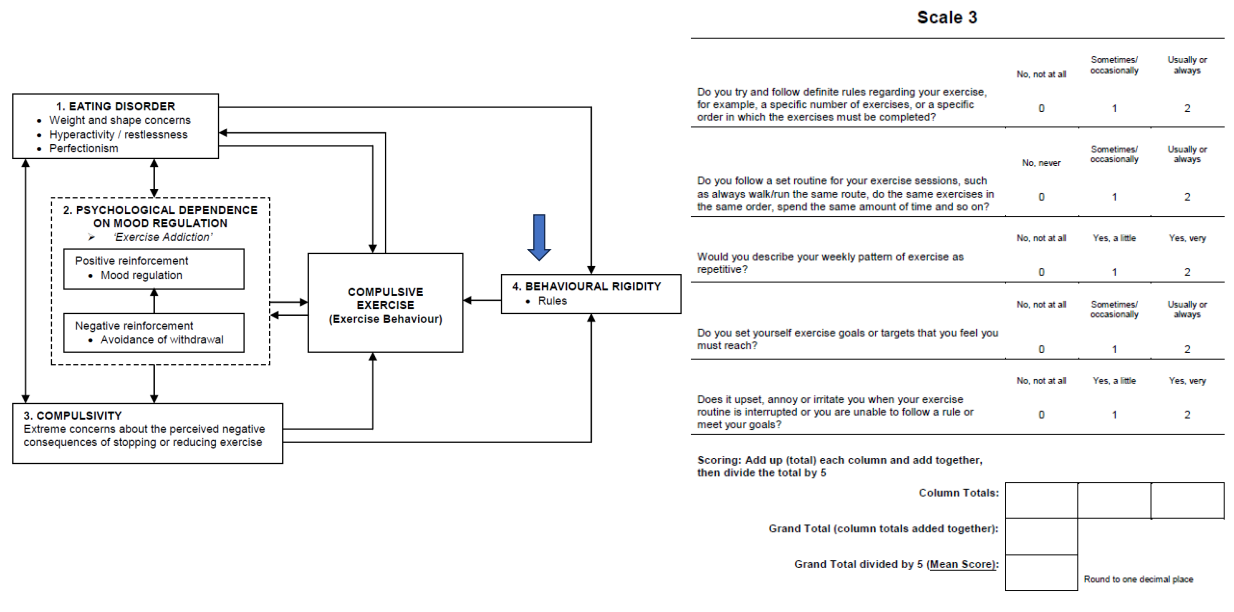
Behavioural rigidity
This scale measures how rigid and repetitive exercise behaviour has become.
A high score:
Exercise behaviour (routine) has become very rigid and repetitive, and strongly predicts that a patient will have great difficulty in cutting down, stopping, or even altering their exercise behaviour.
Associated with the following of specific „exercise rules‟ (e.g. “I must exercise for at least xxx hours”).
.A mid-range score:
Patient would be able to cut down, stop, or alter the exercise behaviour without too much difficulty so long as it is carefully planned.
A low score:
A highly flexible approach to exercise, as they do not follow any sort of fixed routine or rules.
Compulsive exercise
This scale measures how compulsive a patient has become about exercise.
A high score:
Exercise has become grossly over-inflated in terms of its importance, and as such a patient feels that they „have‟ to exercise.
Patient may hold false beliefs about the importance of exercise for your general well-being and health -> very difficult to cut down or stop your exercise behaviour.
Very concerned (afraid) of what may happen to them if they stop or cut down your exercise (i.e., the negative consequences).
This scale is one of the strongest indicators of an „unhealthy‟ approach to exercise, and as such a high or mid-range score on this scale is very likely associated with high scores on many of the other scales, especially scales 2 and 3.
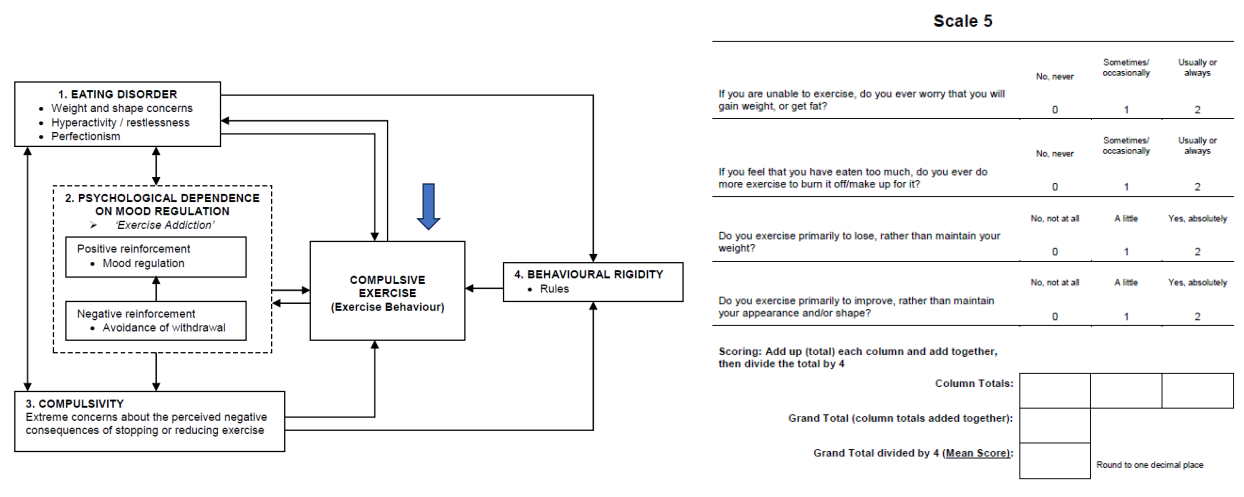
Weight and shape concerns
This scale measures how obsessional a patient has become about exercise specifically in terms of its influence on weight and shape.
A high score:
Exercise primarily for weight and shape reasons -> a very strong reciprocally reinforcing relationship between exercise and eating, attitudes, beliefs and behaviours (i.e. the exercise attitudes, beliefs and behaviours are supporting the eating disorder and vice-versa).
Exercise attitudes, beliefs and behaviours are a significant maintenance factor for the eating disorder, and strongly suggests that they may hold false beliefs about what constitutes appropriate and „healthy‟ exercise.
Even in the absence of an eating disorder, a high score on this scale would indicate an extremely un-healthy approach to exercise, due to the grossly inflated importance attributed to its influence on weight and shape.
A mid-range score:
Exercise largely for weight and shape reasons, and in the presence of an eating disorder suggests a moderately strong reciprocally reinforcing relationship between exercise and eating, attitudes, beliefs and behaviours.
A low score:
Shows that weight and shape are not primary reasons for exercise.
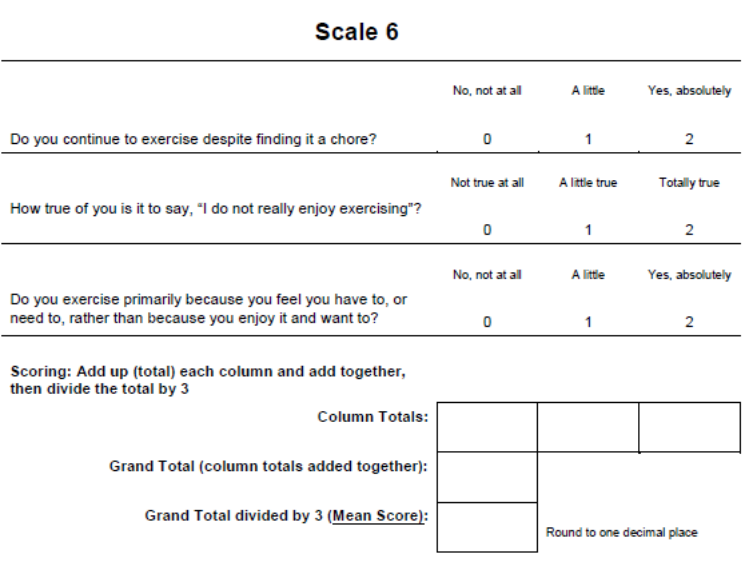
Lack of exercise enjoyment
This scale measures how un-enjoyable exercise is for the patient.
A high score:
A patient does not enjoy exercise at all, and strongly suggests this patient is exercising for the wrong reasons.
A mid-range score:
Does not always enjoy exercise, they do not hate it.
A high or mid-range score on this scale would therefore suggest that if they have had a high score on any of the other scales, they should make efforts to re-learn what constitutes „healthy‟ and enjoyable exercise so that they may continue to exercise in a manner that improves their health and well-being.
The subsequent sessions
Integrate home-tasks in your multi-component physiotherapy approach
Homework serves as both an introduction to each session and the primary education component, and should be thoroughly reviewed.