Exercise volume is high (between 2 and 7+ h daily).
The high volume of exercise, and its negative impact, is minimized by the individual.
Other things in life must fit around exercise. Exercise is judged to have primary importance in life.
The structure of exercise undertaken is rigid.
Exercise is often undertaken in the course of routine activities (e.g., push ups at work).
Desire to increase.
The person is often preoccupied with exercise (e.g., having persistent thoughts of when and where next session will take place, planning training, thinking of ways to exercise during other activities).
Exercise volume has increased over time in order to avoid negative feelings of guilt or laziness.
Exercise is used as a way to cope with negative life experiences or stressors.
Negative affective response when exercise is reduced or sessions are missed/stopped (withdrawal symptoms).
Attempts to reduce exercise volume are feared and/or unsuccessful.
Feeling of guilt when exercise is missed or reduced.• Lies about or minimizes time and intensity of exercise.
The exercise behaviour has jeopardized or resulted in a loss of e.g. a significant relationship, job, or educational or career opportunity: social / occupational impairments.
Despite rational understanding of the negative physical and/or psychological burden of exercise habits, habits are continued.
Exercise is continued in spite of illness, injury or severe pain, at levels beyond rehabilitative training: not listening to the body.
Rapid return to high exercise volume following a period of abstinence.
Coached athletes train beyond what is prescribed by trainer
What about excessive exercise in professional athletes: is it compulsive or an addiction?
While professional athletes (as opposed to fitness and recreational exercisers) report equally high or even higher scores on exercise addiction questionnaires, compared to other exercisers:
They are very unlikely to have lost control of their behaviour.
They are unlikely to exercise beyond what is required to excel at their sport.
They will also, by necessity, recognize the benefits of recovery to improve performance.
What about patients with eating disorders?
It is clear that excessive, compulsive exercising plays a role in a number of eating disorder types = secondary exercise addiction.
It is also possible that in individuals who are addicted to exercise, disordered eating patterns emerge later.
Prevalence rates reported in the literature
In the general population: <1%
In people with eating disorders: 38-45%
Potential causes of exercise addiction
Biological factors:
Genetic predisposition and / or chemical imbalances in the brain (e.g. dopamine receptor genes – reward system signalling)
Psychological factors:
Low self-esteem, body image issues, perfectionism, and a desire to gain control over one's life can contribute to compulsive behaviour.
Sociocultural pressures:
Cultural emphasis on fitness, appearance, or athletic achievement may contribute to unhealthy exercise habits.
Sociocultural Pressures
Those with compulsive exercise behavior often are extremely invested in the appearance ideal and may have difficulty letting go of this pursuit.
It is useful to make a distinction between the appearance ideal and the healthy ideal.
The appearance ideal is often about appearing ultra-slender. People often engage in very unhealthy behaviours to attain this slenderness, including going to extreme ends.
In contrast, the healthy ideal is about striving for a healthy body, which is typically nowhere near as slender as the appearance ideal.
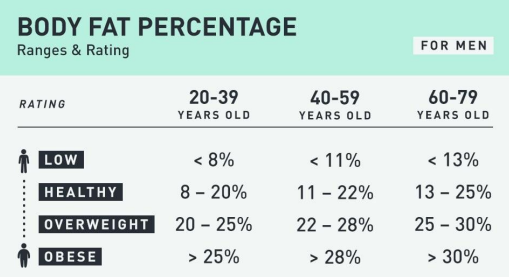
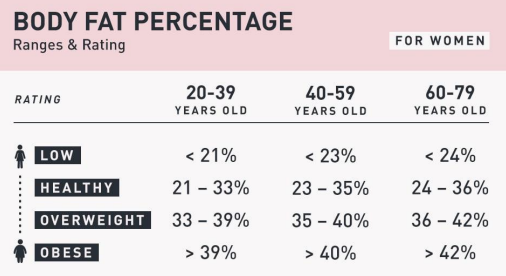
What is a healthy body fat percentage for men and women?
A healthy body is not defined by being fat-free, but by having the right balance—essential fat supports hormones, brain function, and overall well-being.