- Possible causes for a 25 year old
- electrical problems, structural heart diseases, genetics, drugs
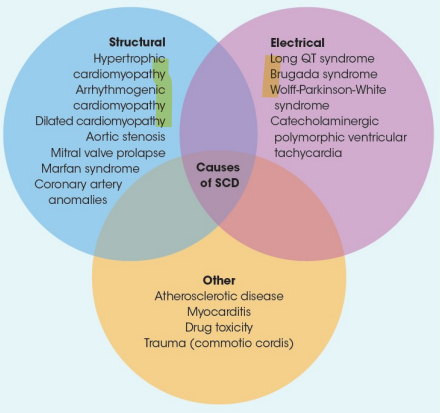
- electrical problems, structural heart diseases, genetics, drugs
Hypertrophic Cardiomyopathy
- Prevalence:
- 1/500 in general population
- 1/2000 in athletes
- Cause of SCD in 2-36% of cases in athletes
- Heterogeneous genetic disorder resulting in asymmetric LV hypertrophy, myocardial disarray on histology and fibrosis
- Variable penetrance with some never developing phenotype of HCM
- Might be asymptomatic for long time ->screening needs to continue until young adulthood
Symptoms
- SCA (80% of the time) - risk is higher with intense exercise
- dyspnoea on exertion
- atypical or anginal chest pain on exertion
- presyncope and syncope
- particularly during or immediately following exertion
- palpitations
- fatigue
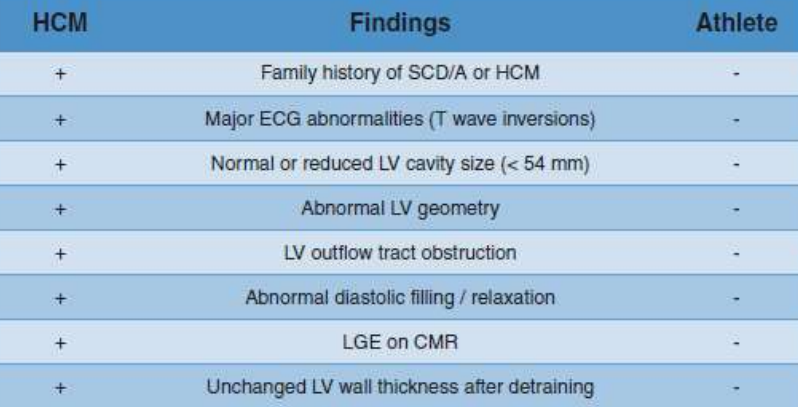
Diagnosis
- ECG - abnormal in 90-95%
- P-wave abnormalities
- Left axis deviation
- Deeply inverted T-waves ‘(V2-V4)
- Pathological Q-waves – reflective of septal depolarization
- High QRS voltages
- ST-depressions
After the diagnosis
- No cure, but focus on prevention of complications/adverse events
- Risk factors for SCD in patients with HCM
- Unexplained syncope
- Family history of SCD
- Severe LVH (> 30 mm)
- Sustained or non-sustained VT
- Attenuated BP response to training/testing
- low positive predictive value, high negative predictive value
- ICD
- ICD
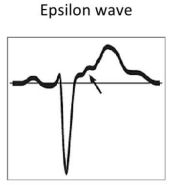
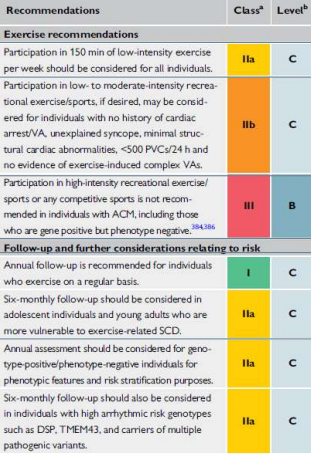
Arrhythmogenic Cardiomyopathy
- Prevalence: 1/1000 – 1/5000 in general population
- Cause of death in 3-29% of athletes
- Progressive inherited heart muscle disease characterized clinically by ventricular electrical instability and pathologically by progressive loss of myocardium with subsequent myocyte death and fibro-fatty scar
- Exercise causes progression of the disease
- Risk of SCA: 2-5 times higher in competitive athletes vs recreational or non competitive sports
Symptoms
- Exercise-induced palpitations
- Presyncope
- Syncope
- Shortness of breath
- Sudden Cardiac Death
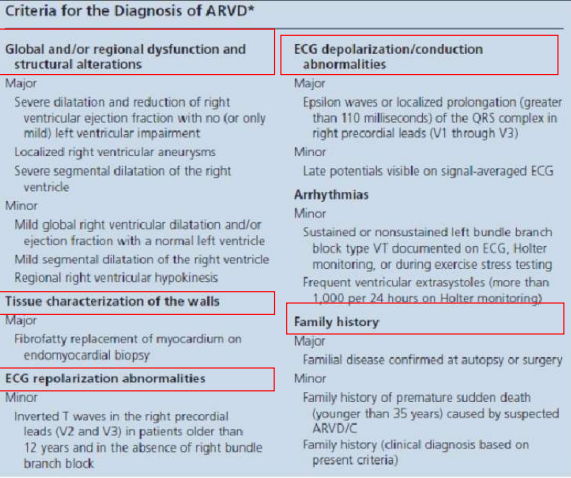
Diagnosis
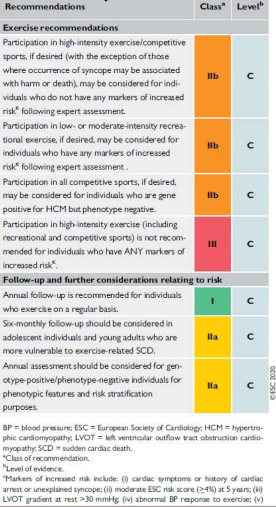
Recommendations
Commotio Cordis
- Sudden cardiac arrest triggered by a blunt, nonpenetrating, and often innocent appearing blow to the chest, without damage to the ribs, sternum or heart and in the absence of underlying cardiovascular disease
- 2nd leading cause of SCD in athletes in US
- Male > female
Important Variables and Mechanism
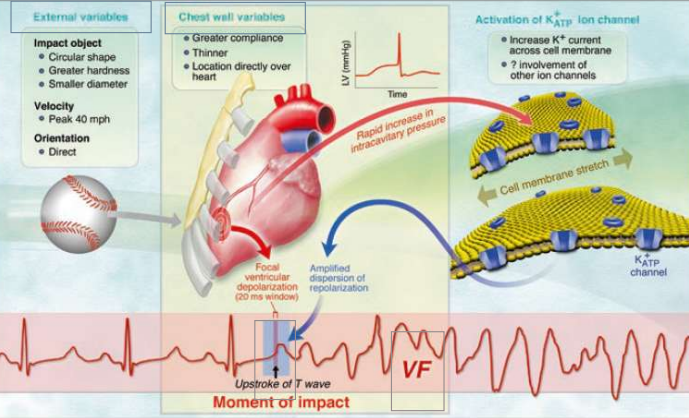
- Primary prevention
- avoidance of chest blows
- chest wall protection
- softening the ball
- Secondary prevention
- increased recognition that a person is in cardiac arrest
- early CPR and defibrillation
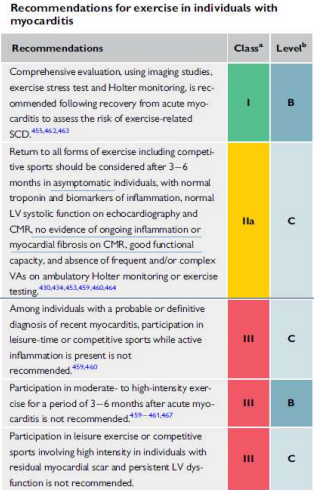
Myocarditis
- Acute inflammatory process of the myocardium
- Caused by variety of infectious agents, systemic diseases, drugs, toxins
- 2-31% of SCD in athletes
- Associated with
- atrial and (lethal) ventricular tachyarrhythmias, bradyarrhythmia
- dilated cardiomyopathy
- Suspicion in:
- Individuals with systemic viral symptoms
- Developing cardiac-related symptoms
- Vigorous exercise might accelerate and worsen myocardial affectation in systemic viral and autoimmune processes
- Primary prevention
- restriction of sport in case of infection (neck check) and systemic symptoms (fever, myalgias, diarrhoea, elevated resting heart rate)
- Education - Avoidance of recreational drugs or doping agents
Recommendations
Coronary Artery Anomalies
- Coronary arteries arising from an anomalous sinus in the aortic root
- Left coronary artery origin in right sinus of Valsalva
- Right coronary artery origin in the left sinus of Valsalva
- 0.5-1/100 of all healthy individuals
- 4-16% % of SCD in young athletes
- Clinical manifestation
- With or Without hemodynamic consequences
- Usually asymptomatic
- If symptoms: angina, syncope, presyncope
- Difficult diagnosis: MRI, CT angio
- Therapy: surgical correction
- Wolff-Parkinson White syndrome (A)
- Most common abnormal finding on ECG in screening programs
- 1/1000 in population has WPW
- Tachyarrhythmias due to an accessory pathway (bundle of Kent)
- Short PR, delta waves (slurred QRS upstroke), widened QRS
- Palpitations, syncope, near-syncope, SDC
- Therapy: ablation
- Long QT syndrome
- Ion channelopathy
- 1/2000-1/5000
- Qtc > 400ms (470 athletes) in males and > 460 (480 athletes) ms in females
- Return-to-sport: shared decision
- ICD if
- History of SCD – recurrent syncope and polymorphic VT despite B-blocker therapy
- Brugada syndrome
- Ion channelopathy - ICD
- Syncope/ SCD during SLEEP
- Coved-type and downsloping ST-segment Elevations (V1-V3)
- Return-to-sport: shared decision