Patient overview
- Name: Anna
- Age: 35
- Occupation: Teacher
- Presenting complaint: Chronic lower back pain for 5 years, increasing intensity over the past 3 months.
- Medical history: No major surgeries or fractures; occasional episodes of anxiety.
- Social history: Recently separated from an abusive partner, living with two children. She reports ongoing feelings of stress and emotional distress.
- Previous treatment: Anna has not received any formal treatment for her back pain. She has tried various self-care measures (e.g., stretching and over-the-counter medications) with minimal relief.
Trauma history
- Trauma history: Anna reports experiencing emotional and physical abuse from the past relationship. She does not report severe PTSD symptoms but experiences occasional anxiety and stress linked to her past relationship.
- Psychological impact: Anna mentions occasional hyperarousal symptoms (e.g., feeling tense or irritable) when faced with stressful situations. She does not feel that the recent break-up is the primary cause of her back pain but acknowledges it could be contributing to her overall stress levels.
- Physical impact: Anna experiences ongoing lower back pain, which she believes worsens during stressful times. She also feels stiff and tight, especially in the morning or after long periods of sitting or standing.
Initial assessment
- Physical assessment:
- Posture: Mild forward head posture and slight thoracic kyphosis.
- Range of motion: Limited lumbar flexion (pain reported at 40 degrees), with discomfort intensifying with forward bending.
- Palpation: Tenderness over the lumbar paraspinal muscles, especially on the right side.
- Special test:
- Straight leg raise test: Mild discomfort at 40-45 degrees on the right side.
- Prone knee bend test: Mild tension in the right hip flexor region.
What could happen in patients who feel uncomfortable, mainly triggered to their past (traumatic) history?
- These tests can sometimes feel unsafe or threatening because of:
- Body positioning: lying supine or prone can evoke a sense of vulnerability or loss of control.
- Physical exposure: even minor lifting of clothing, or a therapist being physically close, can be triggering.
- Sensations: the stretch, discomfort, or pain might mimic sensations associated with past traumatic experiences.
- Power dynamics: the therapist guiding or holding their body may bring back feelings of being controlled.
- Possible reactions patients might experience
- Psychological: anxiety, panic, flashbacks, dissociation, emotional shutdown, or sudden crying/laughter.
- Physiological: increased heart rate, sweating, shaking, holding breath, or muscle guarding.
- Behavioural: pulling away, abruptly stopping the test, or becoming withdrawn and less communicative.
- Clinical consequences:
- Reduced trust in the therapist or healthcare system.
- Avoidance of future sessions or assessments.
- Exacerbation of symptoms if the experience reactivates trauma-related distress.
Trauma-informed considerations
- Explain the purpose of the test in advance and get explicit consent.
- Offer choice (e.g., “Would you prefer we skip this test today?” or “Would you like to position yourself?”).
- Check in during the test for comfort and readiness.
- Modify or adapt (e.g., do the test in side-lying, use active rather than passive movements, or rely more on history and functional tests if appropriate).
- De-brief afterwards if the patient seems unsettled.
Essentially, what could happen is not just a false-positive/negative on the test result, but a reactivation of traumatic memory with potential harm to the therapeutic relationship and the patient’s psychological safety.
Modify or adapt the straight leg raise test:
- Start with a smaller range of motion and gradually increase based on Anna’s comfort level
- Perform the test slowly and explain the movement at each step.
- Ensure Anna feels in control of the process by asking her if the movement feels okay at each stage.
- If Anna experiences discomfort or emotional distress, stop immediately and offer reassurance.
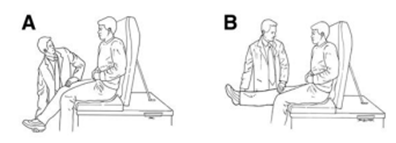
- You can do the test also seated
Modify or adapt the prone knee bend test:
- Perform the test with Anna in a seated position rather than lying prone to avoid feelings of vulnerability.
- Check in with Anna about her comfort level, making sure she feels safe throughout.
- Use a gentle range of motion and avoid applying too much pressure to prevent triggering emotional distress.
Proposed trauma-informed approach
- Establish rapport:
- Spend time listening to Anna’s concerns, building trust, and explaining the purpose of the treatment. Begin the session by checking in with her about her comfort level and asking if she has any specific concerns about physical touch or movements during the assessment.
- Explain treatment steps:
- Clarify each part of the assessment and treatment plan, including why certain movements are necessary, such as the Straight Leg Raise Test and Prone Knee Bend Test. Always ask for her consent before proceeding.
- Modify assessment techniques if needed
- Gentle movement:
- Begin with low-intensity exercises such as gentle stretching and mobility work for the lower back, focusing on breathing and relaxation. Avoid any positions or movements that feel invasive to Anna, like lying flat on her back for extended periods.
- Incorporate psychological safety:
- Throughout the session, keep the communication open, regularly checking on Anna’s emotional state and asking for feedback.
What specific communication techniques can the physiotherapist use to ensure Anna feels heard and understood throughout her treatment?
To ensure Anna feels heard and understood throughout her treatment, the physiotherapist should use the following trauma-informed communication techniques:
- Establish trust and provide choice
- Obtain informed consent at every step:
- Before performing any assessment or treatment, explain the purpose and ask if she is comfortable proceeding.
- Give Anna control:
- Allow her to set the pace of the session and offer options.
- Obtain informed consent at every step:
- Use clear, non-threatening language
- Avoid medical jargon:
- Explain concepts in a way that Anna can understand
- Validate her experience:
- If Anna expresses discomfort, acknowledge it without dismissing her concerns
- Avoid medical jargon:
- Active listening and empathy
- Use reflective listening:
- Repeat key points back to Anna to show understanding.
- Acknowledge her emotions
- If Anna expresses frustration or fear, respond with empathy
- Use reflective listening:
- Be aware of non-verbal clues
- Monitor Anna’s body language:
- If she tenses up, avoids eye contact, or seems anxious, check in with her.
- Adopt an open, relaxed posture:
- Avoid standing over Anna or using a dominant stance. Maintain gentle eye contact and sit at her level when possible.
- Monitor Anna’s body language:
- Reassure and normalize reactions
- Acknowledge trauma without focusing on it:
- If Anna shares her trauma history, acknowledge it without forcing further discussion
- Reframe pain and progress positively:
- Help Anna see small improvements without invalidating her experience.
- Acknowledge trauma without focusing on it:
- Encourage two-way communication
- Ask open-ended questions to encourage detailed feedback.
- Check in regularly:
- Ask throughout the session if she is feeling okay and offer alternatives if needed.
Trauma-informed communication
Most important communication strategies:
- Explain every step:
- Ensure Anna understands what will happen during each session and give her control over the process.
- Use empathy:
- Acknowledge Anna’s emotional state.
- Watch for non-verbal cues:
- Stay attuned to Anna’s body language for signs of discomfort or anxiety, such as tense posture or shallow breathing.
Summary:
By using trust-building, clear language, active listening, non-verbal awareness, reassurance, and two-way communication, the physiotherapist can create a safe and empowering environment for Anna. This approach not only supports trauma-informed care but also enhances patient engagement and long-term treatment success.
Progress and adjustments
- Treatment progress:
- Anna reports slight improvement in her lower back pain but mentions feeling tense during certain stretches.
- She also expresses a desire to avoid exercises that involve lying on her back, as it feels vulnerable for her.
- Anna reports difficulty managing stress and anxiety outside of sessions.
- Proposed adjustments:
- Change exercises:
- Incorporate more standing or seated exercises to avoid positions that trigger vulnerability.
- Introduce stress management techniques:
- Consider introducing mindfulness or breathing exercises to help manage stress and anxiety.
- Referral to mental health support:
- Given there are no clear indications for PTSD symptoms, a referral to a mental health provider specializing in trauma might not be the first option - > assess.
How can the physiotherapist ensure Anna’s treatment remains trauma informed as she progresses through rehabilitation? What strategies can be introduced to address her stress and anxiety in conjunction with physical recovery?
Key clinical considerations
Takeaways based on Anna’s story
- Trauma-informed care is about more than just physical rehabilitation; it’s about creating a supportive, empathetic environment where patients feel safe to heal both physically and emotionally.
- Modify treatment and communication based on individual patient histories to foster trust and maximize therapeutic outcomes.
- Always be aware of subtle signs that a patient may be experiencing distress and be ready to adjust your approach accordingly.