- Ms DD, 24 years old, primary school teacher, is referred to the syncope outpatient unit after previously falling unconsciousness in the waiting room of your practice, after which she was admitted to hospital with a subdural hematoma. She recovered fully with conservative treatment
- Elements of the case:
- She was sitting in the waiting room, texting when you entered the room.
- She lost consciousness while she was getting up to stand.
- She fell forwards onto her head.
- She possibly felt light-headed/dizzy shortly beforehand - unclear???
Important: More items from her case history
- Past personal history: nothing of significance, no previous events
- Before the event: She didn’t feel unwell that day. Sometimes during exertion she feels some heart palpitations when she cycles hard. She can’t remember who she was texting. Just before the collapse she didn’t feel anything abnormal.
- During the event: she lay on the ground and there were five uncontrolled jerking movements of her hands and feet. Afterwards, she was alert as before, but she had a severe headache.
- After the event: she came round lying on the floor of your waiting room. No nausea, no sweating. No tongue biting, no muscle pain.
This is T-LOC, because
- A state of real or apparent loss of consciousness
- Lack of response to sensory stimuli & abnormal motor control
- Complete unawareness, characterized by amnesia for the period of unconsciousness
- Rapid onset
- Short duration
- Spontaneous complete recovery
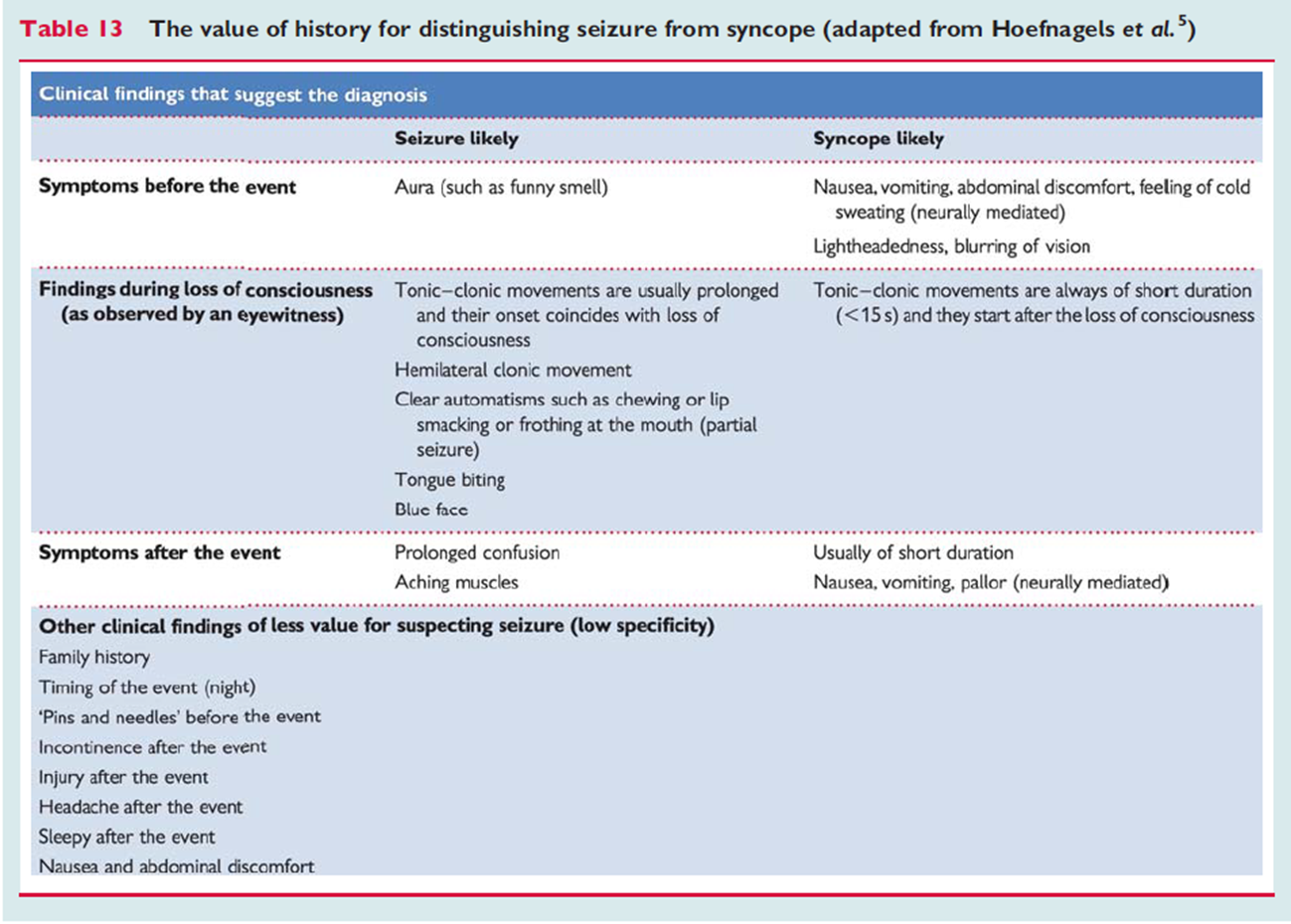
Type of T-LOC
- Not epileptic -> no sensory stimuli, responsive to trigger
- epileptic is more chaotic and lasts longer
- Not psychogenic pseudosyncope -> lasts longer than syncope, difference with eyes are closed most of the time in pseudo
What would you like to know next?
- Nothing: you are now quite sure it is benign and no further investigation is needed
- Family history
- An uncle is said to have died young while swimming, though that’s something she heard. Her father and brother of her father once did an exercise stress test, she does not remember/know the reason for that (never asked).
- Something else
Now the patient history is complete and the physical examination and ECG can be done
- HR: 75 bpm
- Blood pressure:
- Office sitting 115/87
- Office standing 123/85
- No abnormalities found over heart and lungs
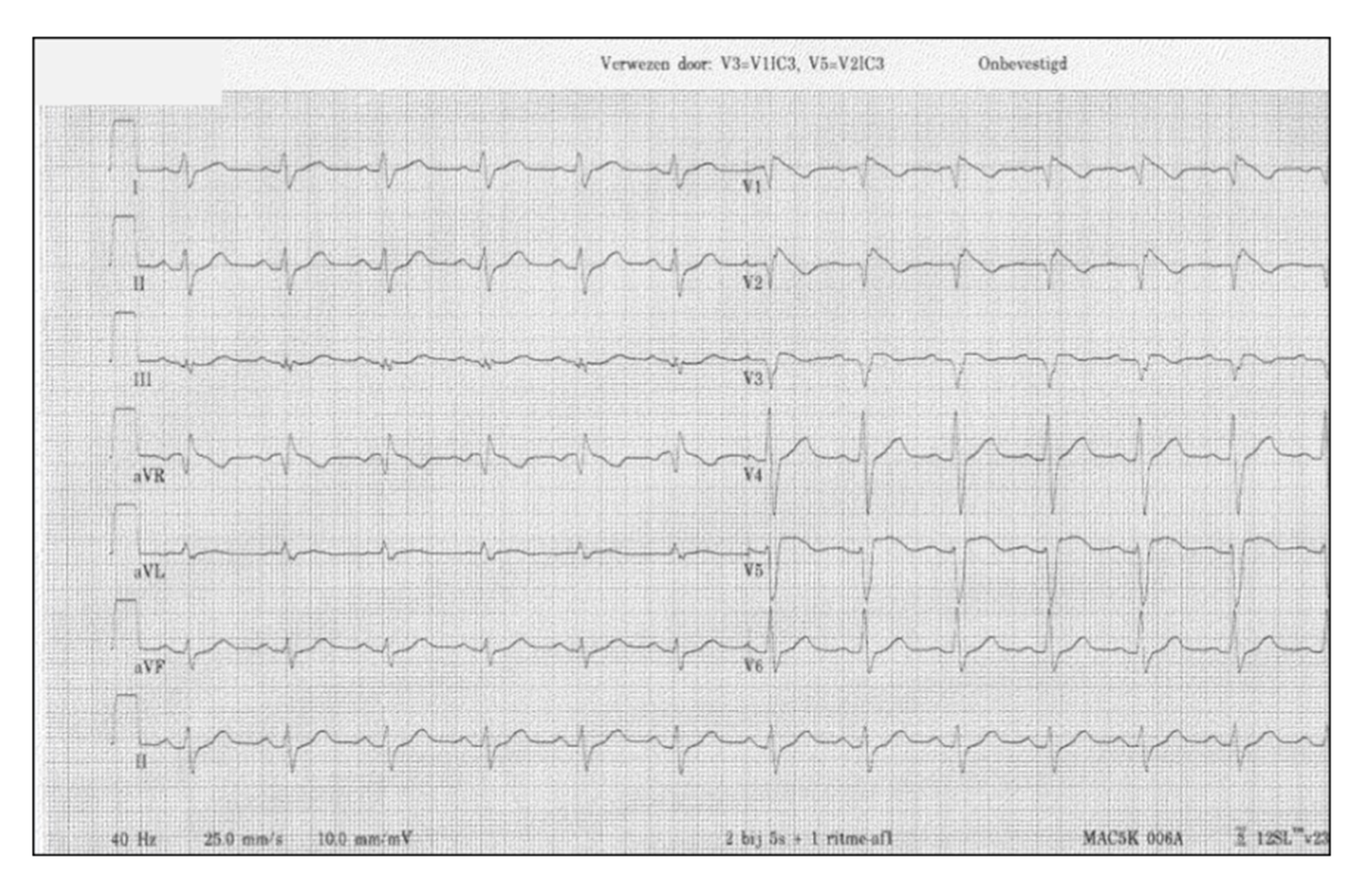
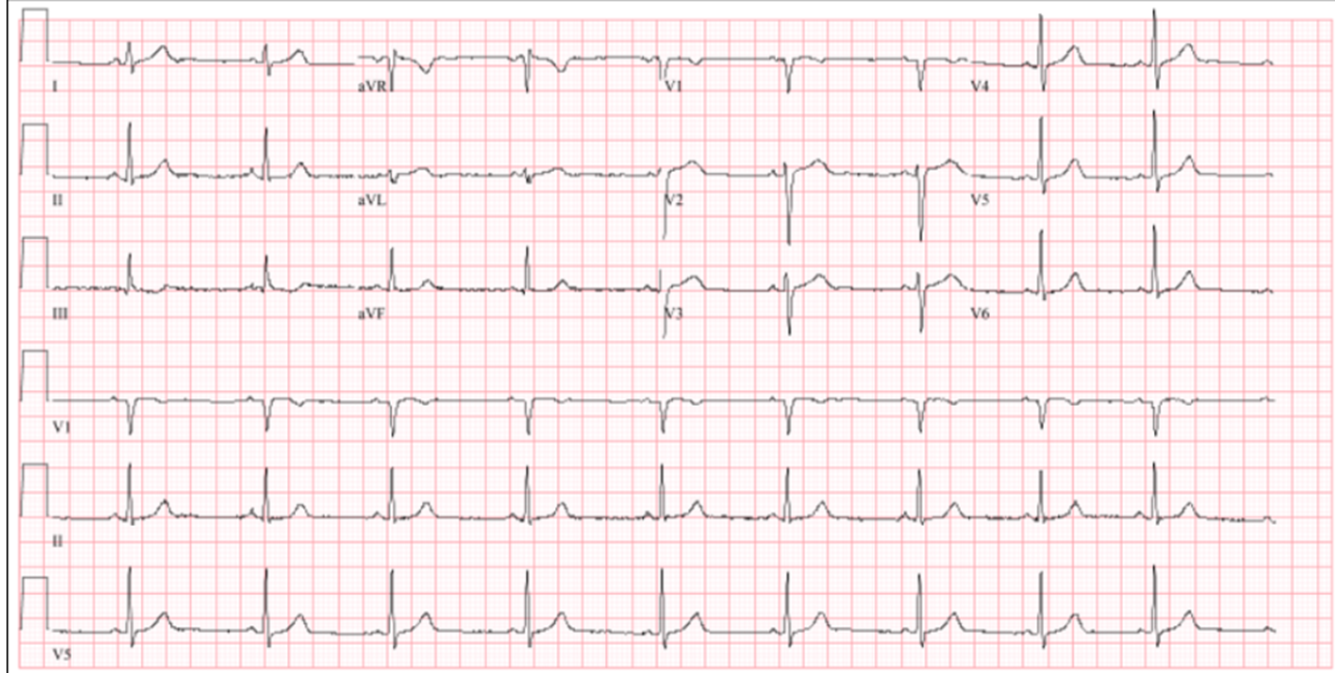
- Resting ECG?
What type of syncope?
- Cardiac - can be
Which elements of the case do you consider to be alarm symptoms?
- Family history is positive for sudden cardiac death
- She lost consciousness
- She was severely wounded
- The ECG is normal, but that doesn’t mean anything
- She collapsed at a young age
- She did not remember feeling light-headed
- Heart palpitations on exertion
- It happened before she was actually standing
Which is the most common cause of SCD in young people?
--> Brugada syndrome