Two-stage screening processes, where depression is assessed first and suicide risk is only explored if a person screens positive, have significant limitations. It can result in an acceptable number of false negatives, as suicidal thoughts can occur in the absence of clinical depression
Physiotherapists should be attentive to the signs of psychological and suicidal distress, particularly when working with high-risk populations such as people living with chronic pain, long-term disability or other complex health conditions
Some people may feel uncomfortable disclosing suicidal thoughts when asked for formulaic or scripted questions that feel inauthentic, especially if they fear that such disclosures could trigger a health professional response that threatens their autonomy
A pragmatic approach is integrating it in your conversation by normalising mental health issues
If you want to use a questionnaire, normalise it…
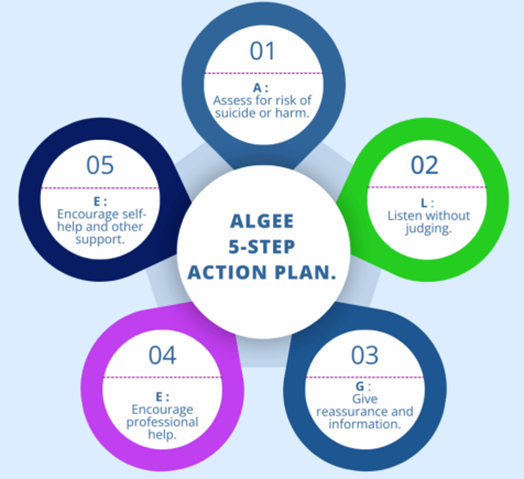
L: Listen nonjudgmentally
Show empathy while they share
Avoid interrupting or dismissing their feelings (‘it’s not that bad’ can be harmful)
G: Give reassurance and information
Three potential reassurance response you could give:
Normalising and validating
‘It makes sense to feel overwhelmed given everything you’ve been going through. Many people feel this way when facing ongoing pain.’
Hope-oriented reassurance
‘Even though it feels hopeless now, there are ways to manage both your pain and your mood. Support is available, and it can make a real difference.’
Empowering reassurance with guidance
‘Reaching out like you did is a really strong step. There are professionals who can help you through this, and we can work together to make a plan, so you feel safer and supported.’
Or a combination of these
E: Encourage appropriate professional help
Suggest seeing a GP or psychologist if needed
E: Encourage self-help and other support strategies
Suggest coping strategies compatible with physiotherapy